Anemia in Uganda

Anemia is a critical health problem in Uganda with 53 percent of children and 32 percent of women anemic (UBOS and ICF 2017). This has significant adverse effects on the country’s health and economic development. Anemia is estimated to be the third-leading cause of mortality in children under five years of age (MOH 2016), and it is estimated that anemia in adult women will cost Uganda about 1.1 trillion Ugandan shillings (US$445.3 million) in lost productivity in the period 2013–2025 in the absence of appropriate investments (Namugumya et al 2014).
Anemia is characterized by a low concentration of hemoglobin in the blood. Although the exact causes of anemia are undocumented in Uganda, evidence shows that genetic traits such as sickle-cell anemia and thalassemia, low bioavailability of iron in the diet, malaria, schistosomiasis and hookworm infections, other nutritional deficiencies, HIV, and poor sanitation are important determinants of anemia among children and women in the East African region (Kassebaum 2014).
SPRING’s Approach to Reducing Anemia in Uganda
The United States Agency for International Development’s (USAID’s) Multi-Sectoral Nutrition Strategy 2014–2025 highlights the need for an integrated, multi-sectoral approach to reduce anemia. In the past decade, USAID’s Micronutrient Program (MOST) and Micronutrient and Child Blindness Project (A2Z) projects, as well as the Global Alliance for Improved Nutrition (GAIN), have supported the Government of Uganda (GOU) in addressing anemia. MOST strengthened guidelines and programs for maternal anemia at the national and district levels, and integrated deworming, malaria prevention, and iron–folic acid (IFA) supplementation into facility-based antenatal care. A2Z carried on MOST’s efforts, improving coverage and adherence to anemia interventions for pregnant women. A2Z also worked with GAIN to support the government in fortifying wheat flour, maize flour, and vegetable oil. Since 2012, USAID’s Strengthening Partnerships, Results, and Innovation in Nutrition Globally (SPRING) project has worked to prevent and control anemia through multisectoral coordination platforms to strengthen policy and programming for anemia and micronutrient deficiencies. SPRING has supported the development of policy documents to guide planning and implementation of programs at the national and district levels. In addition, SPRING supported the enforcement of industrial food fortification regulations and guided the pilot and rollout of home-based food fortification in Uganda.
This brief describes our investments and lessons learned for: 1) multi-sectoral anemia planning and coordination and 2) implementation of nutrition interventions to reduce anemia. We grounded our efforts in three main programming principles:
- Strengthen policy environment
- Improve partnerships
- Build capacity
Multi-Sectoral Anemia Planning and Coordination
SPRING has supported coordination and collaboration for anemia efforts in Uganda, bringing together stakeholders from across sectors at the national and district levels to improve planning and program implementation.
National Anemia Efforts
In 2013, at the request of the GOU, SPRING carried out a national anemia landscape analysis to better understand the factors contributing to anemia and assess the policies and programs in place for prevention and control. The analysis found gaps in the policy and program environment. Most importantly, a national level working group on anemia proposed in the National Anemia Policy of 2002 was never formed. In addition, though the coverage of several anemia- related programs had improved over the past decade—e.g. IFA and vitamin A supplementation, deworming, and bed net use—the analysis found that many women and children were not being reached. In response to the landscape analysis findings, the GOU established the National Anemia Working Group (NAWG). This body has a broader mandate than the preexisting Micronutrient Technical Working Group (MN-TWG), which focused specifically on addressing micronutrient deficiencies.
There is a bit of teamwork at the personal level, that personal friendship that has developed over time. I think that will improve the working relationship between ministries.
-NAWG member
The NAWG, comprised of ministries, academia, private sector, civil society, implementing partners, donors, and multilateral agencies, is responsible for coordinating, planning, implementing, and monitoring anemia initiatives in the country. Since its inception, the body has initiated several activities which have resulted in an enabling policy environment (box 1). The NAWG is effective in coordinating anemia activities with the key factors contributing to its success being: effective communication and sharing information, strong leadership with strategic vision, and emergent working relationships. A challenging dynamic was maintaining a balance in perspective among diverse stakeholders, each with their own priorities, while formulating the national multisectoral anemia strategy. We documented lessons learned that will inform future efforts.
Box 1: Highlights of SPRING’s Support to the National Anemia Working Group, 2013–2017
- Supported development of a working document for 2014–2015, the Anemia Action Plan, which prioritized key anemia-related activities per sector and partner and tracked their progress, which was presented during the NAWG monthly meetings. The action plan laid the foundation for developing the anemia prevention and control strategy.
- Provided technical assistance in drafting the Uganda Anemia Prevention and Control Strategy 2017/18–2021/22, which incorporated contributions from multiple sectors and stakeholders, and included a costed implementation matrix and monitoring and evaluation (M&E) framework.
- Supported a randomized trial study at Mulago Hospital to compare compliance with blister packs versus traditional loose packs of iron–folic acid (IFA) supplements. IFA consumption was high, with no difference based on packaging; however, pregnant women and health workers reported a positive view of the blister packs for improved hygiene, storage, and usability. Because compliance is low in most Ugandan settings, though, these findings may not apply to other parts of the country, which are affected by unaddressed supply and demand issues.
- Held yearly National Stakeholder Meetings bringing together over 100 stakeholders to disseminate landscape analysis results, provide technical updates, and share progress on anemia activities.
- Supported the Bachelor’s in Medical Education (BME) Curriculum at Mulago Health Tutor’s College, creating a module for pre- and in-service teachers with anemia knowledge and skills to train health professionals.
Lessons Learned
- A multi-sectoral, collaborative process to develop the country’s first anemia strategy drew feedback from relevant sectors and obtained high-level political commitment, resulting in a country-owned and context-specific document.
- Regular working group meetings fostered networking opportunities, stronger working relationships, and increased collaboration. For example, the education and health sectors worked together to create a curriculum on anemia prevention and control, and the trade and agriculture sectors collaborated to strengthen efforts for vitamin A–fortified bananas.
- Increased understanding of anemia and the role each sector can play to address anemia has contributed to a shift in the country’s approach—from predominantly health sector involvement to inclusion of non-health sectors with key roles at policy and implementation levels.

District Anemia Efforts
Recognizing the need to build district capacity, the NAWG piloted the District Assessment Tool for Anemia (DATA), which was developed by SPRING to help district personnel better understand anemia, analyze its primary causes, and prioritize activities to address anemia in their district. DATA is an Excel-based tool where data is entered and transformed into dashboards during a two- day facilitated district workshop involving sectors related to anemia prevention and control. The NAWG piloted DATA in three districts, selected to include a range of diverse contexts: Namutumba in East Central region has high anemia prevalence and is a SPRING pilot district for home fortification; Arua in West Nile region has high anemia prevalence and is a border district with refugee communities from Democratic Republic of Congo; and Amuria in Eastern region has moderate anemia prevalence, has collected biomarker data on anemia and vitamin A deficiency, and is a World Food Programme pilot district for home fortification. After a successful pilot phase, the NAWG and SPRING partnered with the USAID Regional Health Integration to Enhance Services in the Southwestern region (RHITES-SW) project to roll out DATA in 15 districts to strengthen their efforts to improve stunting and anemia.
District-level stakeholders found DATA to be a useful planning tool and helped them to launch a multisectoral response to addressing anemia. Heads of departments from relevant sectors—agriculture, nutrition, education, disease control, reproductive health, water and sanitation—along with cross-cutting sectors (gender, local development), mapped out activities and timelines to integrate anemia activities into district plans and budgets for the 2017-18 fiscal year. While data management was identified as a main barrier to the use of DATA, districts were mobilized to improve data collection and use, along with periodic use of the tool to assess progress. RHITES-SW committed to providing technical assistance to implement activities and support existing coordination platforms like the District Nutrition Coordination Committees (DNCC) and the District Health Management Teams (DHMT) in tracking and sharing progress.
One of the things I have learned is there are policies that are in place, but as we were trying to pilot this out, you could see that there is a gap in terms of what is happening on the actual ground. I also discovered there was a gap in data. Sometimes there are national figures on certain indicators which are lacking at the district level.
-NAWG facilitator at DATA workshop

Lessons Learned
- NAWG leadership and facilitation at the DATA workshops provided a critical link between the national-level policy context and implementation at the district level. The chief administrative officers, who are appointed by the central government and lead the district-level technical programs, played an important role in providing high-level endorsement. Support from DNCC and DHMT helped coordinate efforts across sectors, and the NAWG initiated a functional change in the DNCC in the districts where we worked with RHITES-SW.
- DATA enabled different sectors to understand how they can work together to address anemia, through increased integration of activities (such as the health and education sectors implementing deworming in schools) and sharing monitoring data to assess progress. SPRING’s mandate to work at the national policy and planning level to reduce anemia, and the mandate of RHITES-SW to reduce anemia and stunting through implementation at the district level, intersected for a successful collaboration and transition for DATA, as well as reflected the importance of continuity as one project phases out and another takes over.
- Integrating DATA into existing district-level structures and building the capacity of staff from different sectors enable a sustainable process through which districts can take ownership in addressing anemia. Workshop participants learned the value of incorporating data from different sectors to inform decision making as well as the need to collect more data to address gaps.

Supporting Implementation of Nutrition Interventions to Reduce Anemia
Anemia reduction requires building evidence and strengthening specific interventions to address the individual causes of anemia. SPRING’s efforts in Uganda focused on industrial and home fortification to reach different target populations.
Industrial Fortification
Industrial fortification of staple foods with micronutrients reaches large segments of the population and improves micronutrient status having an impact on the reduction of anemia (Eichler et al. 2012; Martorell et al. 2015; Barkely et al. 2015). In Uganda, fortification was initiated with a salt iodization mandate in 1994, followed by voluntary and then mandatory fortification of oil, wheat, and maize flour over the next decade.
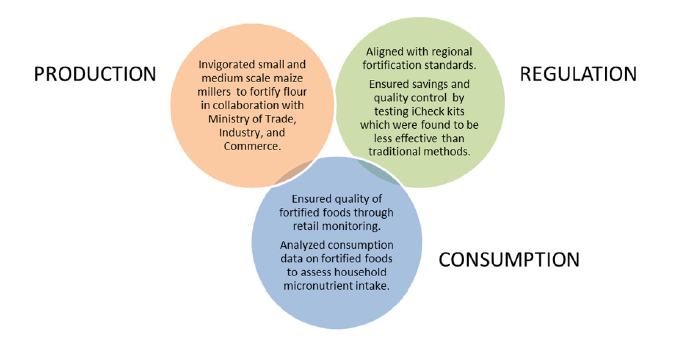
In 2002, the Ministry of Health (MOH) established the National Working Group on Food Fortification (NWGFF), comprised of government, regulatory monitoring bodies, multilateral agencies, food and grain associations, private sector institutions, and academia, to lead fortification initiatives. The NWGFF directs the regulatory agencies that enforce standards and supports the role of the private sector with training to ensure that foods are appropriately fortified. USAID supported the platform through its projects, MOST and A2Z, and SPRING has continued those efforts since 2013. SPRING supported the body’s efforts to improve industrial fortification at all stages of the process, including production, retail, and consumption (figure 1). SPRING also supported development of the National Industrial Food Fortification Strategy 2017–2022, which outlines the roles, responsibilities, and opportunities for both the public and private sectors to prioritize food fortification activities in their work. A key concern for Uganda’s fortification program remains sustainability of enforcement by government regulatory agencies for testing the quality of fortified foods.
Figure 1: SPRING’s Support to NWGFF Efforts
Lessons Learned
- Fortification efforts must take into account regional policies and regulations related to the trade and commerce of fortified foods; this meant that technical support to Uganda’s fortification strategy needed to integrate global best practices, regional standards, and country-specific implementation data collected by the NWGFF.
- The NWGFF has proved an effective platform for creating joint ownership of industrial fortification by the government and private sector. The partnership approach encouraged sharing of experiences between Uganda and other East, Central, and Southern African countries, leading to innovations in fortification technology and testing.
- Our approach of increasing the capacity of private sector producers and government inspectors in parallel was effective in maintaining and institutionalizing the quality of fortified foods.
…They [the health worker] came around telling us that those children under two years should come and get ekilisa kya-baana [nutrients for children, referring to VMP]…When we received the news, we went very fast to the health center and we got them…
-VMP User
Vitamin and Mineral Powders
Micronutrient powders (MNP) are single-dose packets of vitamins and minerals, intended for children over the age of 6 months which are sprinkled onto food before consumption to reduce anemia; in Uganda they are referred to as Vitamin and Mineral Powders (VMP). In 2012, the GOU established the MN-TWG tasked with exploring the introduction of home fortification with VMP in the country. At the request of the MN-TWG, implementing partners— SPRING, the World Food Programme (WFP), and UNICEF—carried out formative research to explore the feasibility and acceptability of VMP. Findings helped to shape a social and behavior change and communication (SBCC) plan, with associated marketing materials including print, radio, and video for use across pilot VMP programs in different districts. Next, the implementing partners carried out complementary pilot studies to investigate the operational requirements for district-level distribution of VMP. Box 2 provides information on the SPRING pilot. The partners developed a national training-oftrainers program and manual and trained six national-level and 23 district-level trainers to roll out trainings for distributors in the pilot districts. They also integrated program monitoring tools into the existing MOH monitoring system. The experiences and findings from SPRING’s pilot as well as those of SPRING’s partners culminated in the development of VMP implemention guidelines, for use in conjunction with the national micronutrient and national infant and young child feeding (IYCF) guidelines.
Box 2: VMP Namutumba Pilot
SPRING’s pilot in Namutumba district examined the cost-effectiveness of VMP through two delivery channels: facility health workers and village health teams (VHT). The study showed substantially higher coverage and adherence to the VMP regimen in the community delivery arm. The community arm had a higher absolute cost, but because program outcomes were better, it was more cost-effective. Participants generally reported positive experience with VMP, but noted challenges related to negative side effects (i.e. diarrhea), child refusal to eat food, and difficulty accessing refills. For the most part, health workers found it acceptable to distribute VMP though there was an added work burden. Messaging for behavior change through multiple channels, as well as regular contacts and quality counseling with beneficiaries and their families, were important for continued use.
| Indicator | Facility Delivery Arm | Community Delivery Arm |
|---|---|---|
| Coverage (eligible children who took VMP in the previous week) | 35% | 64% |
| Average number of packets received during the pilot | 1.5 packets | 2.8 packets |
| Adherence to VMP regimen (one VMP sachet per serving, taking with appropriate foods, and using at least three times a week) | 31% | 58% |
| Cost-effectiveness (cost per sachet per child based on the definition of adhererence to VMP regimen) | $0.59 | $0.24 |
Lessons Learned
- The MN-TWG played an important role in ensuring implementing partners’ activities responded to the needs of the country and efforts were coordinated. This enabled harmonized outputs (SBCC plan, training curriculum, and common monitoring indicators) and forthcoming VMP guidelines that are evidence-based but adaptable to different contexts in Uganda.
- Allowing implementing partners to conduct simultaneous pilots in Uganda using different delivery strategies and studying different outcomes (e.g., WFP assessed biological outcomes and SPRING assessed program costs), generated substantial complementary learning, of value in informing future implementation efforts.
- The MN-TWG built capacity through training of national- and district-level trainers to roll out information in regions and districts. Continuous training and supportive supervision helped maintain reliability of distributors despite high staff turnover in health facilities, and resulted in informal cascade training, which expanded capacity to even more frontline workers.

Building on SPRING’s Legacy to Maintain Momentum for Anemia
SPRING has provided guidance and support to build upon the strong foundation for anemia reduction efforts that can be taken forward by the GOU and implementing partners.
- The three national-level working groups (NAWG, NWGFF, and MN-TWG) have fostered an enabling policy environment for anemia and anemia-related interventions. National anemia and fortification strategies have been developed, with costed interventions as well as an M&E framework. Over the next five years, the GOU can use the indicators and targets in the strategy to track progress and explore further integration of activities across sectors. The strategies need to be disseminated to the district level, and interventions integrated into sectoral work plans and budgets, with support from partners where feasible. In addition, the VMP guidelines provide guidance on implementation approaches, along with harmonized materials and tools. The VMP guidelines can be used by implementers planning to roll out VMP.
- Taking a partnership approach has fostered multi-sectoral engagement and created greater links between the public and private sectors. Future implementation efforts should leverage different partners’ expertise and resources. For example, to support the implementation of VMP programs, one organization can procure the product while another can strengthen the IYCF platform through which VMP are delivered. In fortification, the medium- and small-scale maize millers could adopt new technology to enable fortification of maize flour in small quantities, while regulatory agencies could help millers set up testing facilities to ensure adherence with accepted standards. In addition, as membership is overlapping, working groups can consider merging into one larger coordination body with technical subgroups for specific interventions.
- Building capacity to address anemia at the national and district levels has been successful. The national working groups have improved the capacity of members as they gain knowledge on anemia through technical updates and sharing at meetings. Through use of DATA, the capacity of district implementers has been strengthened to plan for anemia, and the tool can now be expanded to more districts. Using the DNCC and the DHMT structures for rollout will also enhance the capacity of districts for coordinated planning and implementation. Following the implementation of prioritized activities, district efforts should be monitored to assess effectiveness and impact. At the same time, policy makers at the national and district level are now equipped to advocate for further collection and use of anemia-related data for improved programming.
References
Barkley, Jonathon., Kathleen Wheeler, Helena Pachón. 2015. Anaemia prevalence may be reduced among countries that fortify flour. British Journal of Nutrition, 114(2), 265-273. doi: 10.1017/S0007114515001646.
Eichler, Klaus, Simon Wieser, Isabelle Rüthemann, and Urs Brügger. 2012. “Effects of Micronutrient Fortified Milk and Cereal Food for Infants and Children: A Systematic Review.” BMC Public Health 12: 506. doi:10.1186/1471-2458-12-506.
Kassebaum, Nicholas J., Rashmi Jasrasaria, Mohsen Naghavi, Sarah K. Wulf, Nicole Johns, Rafael Lozano, Mathilda Regan, et al. 2014. “A Systematic Analysis of Global Anemia Burden from 1990 to 2010.” Blood 123 (5): 615–24. doi:10.1182/blood-2013-06-508325.
Martorell, Reynaldo, Melany Ascencio, Luis Tacsan, Thelma Alfaro, Melissa F. Young, O. Yaw Addo, Omar Dary, and Rafael Flores-Ayala. 2015. “Effectiveness Evaluation of the Food Fortification Program of Costa Rica: Impact on Anemia Prevalence and Hemoglobin Concentrations in Women and Children.” American Journal of Clinical Nutrition 101: 210–7. doi:10.3945/ajcn.114.097709.
Ministry of Health. 2016. Annual Health Sector Performance Report 2015/16. Kampala: MOH.
Namugumya, Brenda, Kavita Sethuraman, A. Elisabeth Sommerfelt, Lesley Oot, Tara Kovach, and Boaz Musiimenta. 2014. Reducing Malnutrition in Uganda: Summary of Uganda PROFILES 2013 Estimates to Support Nutrition Advocacy. Washington, and Kampala, Uganda: FHI 360/FANTA and Office of the Prime Minister, Uganda.
Uganda Bureau of Statistics (UBOS) and ICF. 2017. Uganda Demographic and Health Survey 2016: Key Indicators Report. Kampala, Uganda: UBOS; Rockville, Maryland, USA: UBOS and ICF.