SPRING/Kyrgyz Republic Formative Research

According to the 2012 Demographic and Health Survey (DHS), 18 percent of children in the Kyrgyz Republic under the age of five are stunted, while 43 percent of children ages six to 59 months and 35 percent of women of reproductive age are anemic. The SPRING project in Kyrgyzstan works primarily in Jumgal rayon of Naryn oblast and 10 jurisdictions of Jalabad oblast. This study was conducted to gain a better understanding of dietary practices of families with children under age two and what factors affect family food consumption, child feeding, and nutrition status. The research was conducted over a period of four weeks in October and November in 2014, immediately following the baseline quantitative survey. The methodology was comprised of six different activities; including focus groups with mothers of young children, key informant interviews with men, a participatory activity with women of all ages, focus groups with Village Health Committees, transect walks with a structured observation guide, and health facility assessments.
Findings of this research are intended to inform SPRING project strategies and communication materials. In general, food insecurity did not appear to be a barrier for most households, but dietary diversity is a serious seasonal issue. Fruits and vegetables are seldom consumed in winter due to scarcity and price. Most women believe that infants need additional water and/or food within a month or two after birth because the mother’s breast milk is not adequate. The first food is most often a gruel made of browned flour, animal fat, and either water or milk. Women do not seem to know the benefits of immediate breastfeeding for themselves, and maternity center staff lack training on the early initiation of breastfeeding. There is also a lack of awareness among women about the appropriate frequency or amount of complementary feeding. While most women start complementary feeding too soon, SPRING baseline data showed that 12 percent of women delay complementary feeding until eight months, believing breast milk is enough food for their child at this time. The cleanliness of a latrine is not a cultural expectation, and only half of mothers properly dispose of small children’s feces. Women in most households have complete mobility and decision-making power to shop for food and seek health services, but mothers-in-law are involved in feeding young children in their households and giving advice to young mothers. Health professionals are perceived as very credible sources of information, providing an opportunity to train them on good counseling skills and build their technical knowledge and capacity.
Key recommendations from the health facility assessment include: collaborating with local government and district health officials to ensure each health facility has the appropriate number of clean, functional latrines or toilets for their staff and patient load; providing all professional health staff training on infant and young child feeding and on anemia, conducting supportive supervision jointly with district health officials; and assisting the Ministry of Health to develop an anemia protocol, including designing a training for health workers on its implementation.
Background
SPRING Project in Kyrgystan
SPRING is a five year USAID-funded Cooperative Agreement to strengthen global and country efforts to scale up high impact nutrition practices and policies and improve maternal and child nutrition outcomes. SPRING provides state-of-the-art technical support and focuses on the prevention of stunting and maternal and child anemia in the first 1,000 days. The project is managed by JSI Research & Training Institute, Inc., with partners Helen Keller International, The Manoff Group, Save the Children, and the International Food Policy Research Institute.
USAID in the Kyrgyz Republic has asked SPRING to improve the nutritional status of women and children within the Feed the Future zone of influence by improving nutrition-related behaviors, enhancing the quality and diversity of diets, and supporting evidence-based nutrition policies. SPRING’s geographic focus is Jumgal rayon of Naryn oblast in the north and 10 jurisdictions of Jalalabad oblast in the south. SPRING’s work plan includes community interventions and mass media to improve nutrition practices at the household level as well as activities to strengthen delivery of nutrition services, including counseling through the health services.
In October and November of 2014, SPRING undertook formative research in the target areas. The findings, combined with additional information gleaned through a baseline survey, will be used to design an effective behavior change strategy with activities, messages and materials for the target population.
Nutrition Issues Identified in the 2012 Demographic and Health Survey
According to the 2012 Demographic and Health Survey (DHS), 18 percent of Kyrgyz children under the age of five are stunted. The prevalence of stunting varies among regions, with the highest prevalence concentrated in the south in the regions of Osh and Batken. No apparent association exists between stunting and wealth quintile or stunting and mother’s educational attainment, and rates of stunting do not differ significantly between urban and rural inhabitants. Just seven percent of women are classified as undernourished, while 31 percent are overweight. Women classified as thin (BMI< 18.5 cm) are more likely to have a stunted child.
According to the DHS, 43 percent of children ages six to 59 months and 35 percent of women of reproductive age have anemia. Anemia prevalence is highest in the regions of Talas and Chui, and lowest in Osh City and Jalalabad regions. As with stunting, there appears to be little association between anemia and wealth quintile or maternal educational attainment, and rates do not differ significantly between urban and rural inhabitants. The DHS reports that only two percent of women took iron supplements for 90 days during pregnancy.
Dietary Intake
Global recommendations suggest that children under the age of six months should be exclusively breastfed, and that children should continue to receive breast milk through the age of two years, with complementary foods introduced at six months of age. Although nearly all mothers in Kyrgyzstan initiate breastfeeding, the DHS indicates that only 38 percent of children are exclusively breastfed at ages 4 to 5 months, the median duration of exclusive breastfeeding is 3.3 months and only 56 percent of children receive breast milk through age two. The findings on infant and young child feeding (IYCF) practices differ somewhat between the DHS and the SPRING baseline conducted in October of 2014 as shown in Table 1 below.
Table 1. Comparison of Infant and Young Child Feeding Indicators, DHS and SPRING Baseline
| Indicators | DHS1 | SPRING Baseline |
|---|---|---|
| % | % | |
| Dietary diversity for children ages 6 to 23 months with emphasis on food sources rich in iron and vitamin A | ||
| Minimum meal frequency for children ages 6 to 23 months | ||
| Minimum acceptable diet for children ages 6 to 23 months | ||
| Early initiation of breastfeeding | ||
| Exclusive breastfeeding from birth through the first six months | ||
| Bottle feeding | ||
| Timely introduction of appropriate complementary foods | ||
| % of children ages 6–23 months who ate foods from four or more groups in the previous 24 hours | 44% | 45% |
| % of children ages 6–23 months who ate iron-rich foods in the previous 24 hours | 61% | 78% |
| % of children ages 6–23 months who ate vitamin A-source foods in the previous 24 hours | 66% | 56% |
| % of children ages 6–23 months who were offered food the appropriate number of times per day for their age and breastfeeding status | 44% | 45% |
| % of children ages 6–23 months who had the minimum adequate diet for their age and breastfeeding status | 16% | 22% |
| % of children who were put to the breast within one hour of birth | 84% | 67% |
| % of children ages 0–5.9 months who received only breast milk during the previous 24 hours | 56% | 32% |
| % of children ages 0–23 months fed anything with a bottle | 22% | 29% |
| % of children ages 6–8 months who received semi-solid or solid food during the previous 24 hours | 57% | 88% |
Context of the Target Areas
SPRING works in one district in the northern province of Naryn called Jumgal where the population is of Kyrgyz ethnicity. The entrance to Jumgal is at the edge of a wide plain, but most of Jumgal is mountainous and along a steep and narrow river valley. There is some irrigation along the river for growing grain and potatoes, but most of the agricultural activity in this area focuses on raising livestock, including sheep, goats, horses, and cattle. The baseline survey reports that, on average, families interviewed have 17 sheep, which is their predominant livestock. Much of Jumgal District is at an altitude of 1,850 meters (6,000 feet) or higher, which means barely three frost-free months and a very short growing season. Livestock are moved to high mountain pastures during the summer. There are several mines in Jumgal where some local men are employed. Few men leave Jumgal to work abroad.
Most of the target jurisdictions in Jalalabad Province are equally mountainous, but with a drier climate. These are also pastoral regions, although people have fewer livestock, and some households have a milk cow. Most families grow potatoes, and some families also grow wheat, which they sell and in turn buy flour to make bread. There are forests in the mountains of Jalalabad, including the world’s largest native walnut forest. Some of the target districts in this zone are isolated four to five months each winter when roads are blocked by snow.
A geographically smaller but more populous portion of the Jalalabad target area is part of a wide, irrigated, heavily farmed valley. This region has a much greater population density and more ethnic diversity, with as much as one-third of the population non-Kyrgyz – primarily Uzbeks, but also Turks, Kazakhs and Russians. There are some enclaves of conservative Muslims. A greater proportion of people in this area have salaried employment either as professionals, skilled laborers, or on large farms, which are former Soviet collectives. At least one-third of households in this area have someone working abroad as either seasonal or longer-term laborers in Russia, Kazakhstan or the Gulf States. Most rural families and those living in small towns have vegetable gardens and fruit trees. In recent years, there has been rural-to-urban migration to the city of Jalalabad, with families living in substandard conditions in deteriorating apartment blocks. The growing season is almost six months with very hot summers. Throughout this report, the area will be referred to as “Lower Jalalabad” to distinguish it from the mountainous areas.
Purpose of the Formative Research
This formative research was conducted to gain a better understanding of dietary practices for families with children under age two, and what factors affect family diet, child feeding and nutrition status, in order to inform SPRING project strategies and communications materials. The formative research was also used to triangulate findings from the baseline survey. The formative research was designed to answer the following questions:
- What do families normally eat in different parts of the target area?
- How is that affected by food availability and food access?
- Which food groups are particularly affected by seasonal availability?
- Does current household food preservation and storage minimize seasonal unavailability?
- Are some nutrient-dense foods available and accessible but underutilized?
- Is there gender bias in intra-household food distribution?
- How much and what food is purchased and what is primarily from home production?
Food Attributes
- Are certain foods perceived as unsuitable for pregnant or lactating women, or young children?
- Are certain foods considered particularly nutritious?
- What do women know about the relative nutritional value of different foods?
- What are attitudes towards foods of low nutrient value?
Infant and Young Child Feeding Practices
- What are attitudes about colostrum, pre-lacteals and immediate breastfeeding?
- What are barriers to exclusive breastfeeding for the first six months of a child’s life?
- When (and how and with what) is complementary feeding started, and when are other liquids introduced?
- Who in the household makes decisions about IYCF practices?
Water Sanitation and Environmental Hygiene
- What is the availability and condition of latrines?
- What are the barriers to maintaining hygienic latrines?
- Are there conditions around houses that expose children to environmental enteropathy?
- What is the access to clean water and who carries water to the house?
Health Facilities
- How well equipped are health facilities to provide nutrition-related services?
- Do health facilities have micronutrient powder (Gulyzak) to distribute? Are iron supplements available in the pharmacy?
- Do health staff have practical knowledge about nutrition?
- Are there any nutrition education materials available for patients to view or take home?
- What are the general conditions of hygiene and sanitation in health facilities?
Methodology

The formative research was conducted over a period of four weeks in October and November of 2014, immediately following the finalization of the baseline quantitative survey which was conducted in late September and early October. A complete schedule of the fieldwork and sites is included in Annex B.
Three members of the SPRING/Kyrgyz Republic staff and one consultant conducted the research, and were assisted in one district by a Peace Corps volunteer. In Jumgal, the two government Health Promotion Unit (HPU) staff were actively involved in leading focus groups and/or taking notes. HPU staff in the two Jalalabad regions assisted in organizing focus groups and interviews, but did not lead focus groups due to a lack of time to train them.
The Health Facility Assessment (HFA) was conducted simultaneously in the same villages by the SPRING Capacity Building Specialist. She always went to the Maternity Center and Family Practice Center for the district and when time allowed, she also visited health facilities in adjacent villages.
Everyone interviewed was read a formal consent statement explaining the purpose of the study and giving them the option to decline to participate. Signed consent forms were collected and have been appropriately filed.
Methods and Tools
Six activities comprised the formative research:
- Focus groups with mothers of young children;
- Focus groups or key informant interviews with men from the community;
- A participatory activity with community women to examine food availability and access;
- Focus groups with Village Health Committees;
- Transect walks with a structured observation guide in communities and district centers;
- HFAs.
The SPRING team and consultant developed guides for each of these activities, adapted primarily from guides used in similar formative research in the region or elsewhere with Feed the Future projects. The guides were translated into Kyrgyz, back-translated and tested before use. English versions of the guides can be found in Annex C. The activities and guides enabled the team to triangulate critical information as well as triangulate findings from the baseline survey. Additional, less-structured opportunistic interviews with individuals filled in gaps in qualitative information.
The HFA tool was adapted from a similar tool used in the USAID Quality Health Care project for prenatal care. The adaptation focused on nutrition-related services of the health system such as anemia, pre-natal nutrition counseling, IYCF counseling, distribution of supplements, and related record-keeping. The HFAs included interviews with health staff, record reviews, and observations.
Team members were given individual training for their assigned activities and worked under the close supervision and guidance of the consultant. After the first day in the field, additional revisions were made to the tools and methods.
Sampling
The first stage of sampling was based on geographic differences. The sample at this stage included Jumgal, lower Jalalabad, and a remote mountain area of Jalalabad, since topography was hypothesized to be a significant factor in food availability and access, together with possible cultural differences in food and child feeding practices between the northern and southern regions of the country. For the second stage, a purposeful sample of nine villages was selected in Jumgal to further capture differences due to topography, physical access, and livelihoods.
Topography was less of a factor in selecting sites in lower Jalalabad than elsewhere, although the purposeful sampling captured one low elevation village and one foothill village as well as urban, peri-urban and rural settlements. One village selected was a former mining town where people do not engage in extensive food production.
Toktogul, the largest mountain district in terms of land area in Jalalabad, was selected to represent the mountain areas because it was still accessible in November from the Bishkek route where the pass is kept open. Villages were purposefully selected in Toktogul to represent both those that are remote and difficult to access, as well as those that are closer to the district center.
Data Management and Analysis
Focus groups and interviews were recorded and transcribed the same day they took place or soon thereafter. Paper copies of notes were typed and shared among the team. Team members debriefed daily and began an initial synthesis of findings. The debriefing helped to further refine the guides and questioning techniques and to identify new threads or additional research questions.
After work in each district or area was completed, team members went through a synthesis process using flip charts to highlight findings. This exercise was completed in English to enable the consultant to begin coding all findings manually. Ultimately, the conclusions coincided completely with those of the initial synthesis.
Key Findings and Implications
Table 2 below highlights key findings and implications from the formative research conducted.
Table 2. Summary of key findings and implications
| Findings from SPRING formative research | Implications and recommendations |
|---|---|
| Factors affecting household food consumption and dietary diversity | |
| Breastfeeding | |
| Complementary feeding | |
| Water, sanitation, and hygiene | |
| Other key findings | |
|
|
|
|
|
|
|
|
|
|
Detailed Findings
Dietary Pattern by Region
Main dishes and hot foods served are almost always mixed foods, such as hearty soups or rice pilaf, or a pastry filled with meat and or vegetables. Soups are generally served in separate bowls, but in the South, variants of pilaf are sometimes served on a single platter from which the whole family eats. Meals are always accompanied by bread and sometimes by vegetable side dishes known as salat (salad), even if the vegetables are cooked. In summer, fresh raw vegetables and fresh fruit are often served at meals and eaten as snacks. The most commonly served fresh produce are tomatoes and cucumbers. Dill, fresh or dried, is used liberally to season food. There is a strong preference for white bread, but if families grind their own wheat, the bread may be whole wheat. Wheat, buckwheat, and other grains are often served as porridge either in the morning or evening.
There are distinct differences in common foods between Jumgal and the whole Jalalabad area, and lesser distinctions between the mountains and the valley of Jalalabad. In Jumgal, due to the predominance of livestock production and the shorter growing season, animal products figure prominently in the daily diet. Rice is much more common in the Jalalabad area and consumption of fruits and vegetables is higher, at least during the autumn season when the baseline survey and formative research were conducted. Table 3 lists the most commonly consumed foods as described by women participating in the formative research, who reached consensus on these food items.
Table 3. Commonly consumed foods in each area
| Jumgal | Lower Jalalabad | Toktogul |
|---|---|---|
| Bread | Bread | Bread |
| Jam | Jam | Jam |
| Milk and milk products – all kinds | Milk products (kefir, yogurt, cream, sary may*) | Milk products (kefir, yogurt, cream, sary may*) |
| Potatoes | Rice | Rice or macaroni |
| Pasta (homemade noodles) | Pumpkin (butternut squash) in season | Pumpkin (butternut squash) in season |
| Meat – chicken, goat, mutton or beef (not daily) | Corn in season Potatoes | Meat – mutton or goat (not daily) |
| Eggs | Sprouted wheat | Butter |
| Wheat drinks without sugar | All vegetables and fruits in summer | All vegetables and fruits in summer |
| Home-canned salads (sautéed vegetables) in winter | Home-canned vegetables or salads | Corn |
| Tea with sugar | Tea with sugar | Tea with sugar |
These results were largely verified by the analysis of dietary diversity for women from the baseline survey (see graph in Annex D), however, the formative research also asked about quantity and frequency of consumption. While the baseline indicates a relatively high level of meat consumption in all areas, formative research participants said that they only consume meat three to four days a week and that the amount put in the usual soup, pilaf, or other mixed dish and shared among all family members is small, about 200 grams. With an average size family of five members, this would be only 40g or less than 1.5 ounce each.
Tea, either black or green, is the universal beverage of choice and is taken with meals and in between meals. Tea is generally sweetened and is given to children. The baseline survey found that a quarter of infants ages 0-5 months were given tea and that increased to almost three-fourths of children between ages 6 and 11 months. This is a concern given the role of tea in inhibiting iron absorption from non-heme sources. Women in the focus group discussions (FGDs) also mentioned that families drink milk and a local beverage made from wheat or corn. Fruit juice with sugar, either homemade or purchased, is generally reserved for special occasions.
Factors Affecting Dietary Diveristy
Food Availability
A wide range of foods is available in all regions. Annex E shows which foods are produced, purchased, consumed on a daily basis, and stored. Most nutrient needs could be met through consumption of locally available foods most of the year, with the exception of vitamin C. Local vitamin C food sources are mostly non-existent in winter months, after all stored cabbage is consumed. People in urban areas have access to shops or supermarkets which import vitamin C-rich foods, however, FGD participants indicated these foods are too expensive for regular consumption. Imported lemons make their way to most market towns, but are used sparingly in tea. The lack of vitamin C is related to the issue of anemia since the vitamin enhances the absorption of any non-heme iron that is consumed.
Red meat is available and is consumed, at most, two or three times a week. Furthermore, the amount consumed by any one family member is small. Families who have chickens report eating more eggs and eating them more often than those who do not have chickens. Egg production from chickens is generally limited, however, since hens are often not kept enclosed or fed well. Households with chickens report frequent epidemics of Newcastle and other possible diseases since there is no longer a vaccination program and the vials of vaccine, when available, are for 100 chickens, which is not practical for smaller household use. The baseline survey reports that the average number of chickens among households who have chickens is six for Jumgal and five for Jalalabad.
There are locally available nutrient-dense foods that are currently underutilized. One of particular note is pumpkin, which grows well in Jumgal. People there report that they don’t know how to use it and often just feed it to their chickens. These pumpkins (cucurbita moschata) keep well long into the winter and are an excellent source of vitamin A. They also grow well in Jalalabad, and people there have various ways of cooking them. Pumpkin leaves as well as from leaves from radishes, beets, and turnips are not consumed at all, but would be a good source of iron and offer some vitamin A as well.
Food Access
Families with cash income eat a much more varied diet than families that produce most of their own food. This was true even in the remote mining communities where food has to be brought in from market towns or purchased in shops. These families reported not only eating more processed food, but also a larger variety of meats and vegetables in particular. In contrast, families with land and livestock but less cash income seem to confine their food choices to what they can produce, purchasing very little except oil, sugar, salt and some foods of low nutrient value such as cakes and instant noodles. In both cases, there does not seem to be much purchasing or trading conducted within communities among neighbors.
The common sentiment about fruit and vegetable purchases is that they are always less expensive in a market town than in more rural areas, and those who live in market towns perceive that produce is cheaper in the next bigger market town, so they sometimes pay for transport to go shopping there. Some women did report that the cost of transport to reach the nearest market or the time involved travelling is a barrier to purchasing fruits and vegetables. On the other hand, professional working women interviewed as key informants in Jumgal mentioned the lack of time is a barrier to purchasing food, particularly to seeking out diverse foods in their local market and shops.
The World Food Programme Food Security Assessment conducted in September of 20132 found that approximately 14 percent of households, primarily day laborers and pensioners, were food insecure. Focus group participants confirmed that these are the groups spending the largest share of their income on food. They mentioned that there is a protective factor in rural households where young couples with small children sometimes live with parents, thus reducing their need to completely depend on their own income for sustenance.
Food Preservation and Storage

Most families contacted in the formative research, with the exception of some urban families, say they store and preserve foods for winter. The foods preserved or stored are fruits or vegetables, including tubers. The formative research did not investigate grain storage since under-consumption of cereal foods is not an issue. In urban households, the main limitation is space, although even some urban households keep tubers, apples, and cabbages in a cold room. They further pointed out that they can buy fresh fruits and vegetables in the market and shops year around, although at high prices in winter.
Foods that are stored rather than preserved include potatoes, cabbages, root vegetables such as carrots and turnips, apples, pomegranates, and pumpkins. According to the baseline, the most common place for storing produce is in a cellar under the house. Potatoes, cabbages, and root vegetables are sometimes buried in trenches and will keep that way for three or four months, with potatoes keeping even longer. This system is quite primitive and all can be lost in severe winters. Apples, pomegranates, some root vegetables and cabbages are sometimes stored in an unheated room, where they will keep for up to three months. Grapes, persimmons, tomatoes and eggplants can be stored in a cool place for up to two months. Families reported that they always consume the stored food by late winter and then must purchase additional potatoes, carrots, and other produce or, if prices are too high, they go without.
The baseline survey asked specifically about what foods are stored and about approximate quantities of those foods. Details are provided in Annex F. The amounts stored are significant. In Jalalabad and some communities of Jumgal, families reported purchasing additional vegetables to store, which implies that home garden production is not sufficient to meet their needs.
Day-to-day food storage is facilitated by the fact that nearly all villages have electricity and most families (85 percent in the baseline survey) have a refrigerator. This has made it much easier for families to store perishable foods such as meat and dairy products as well as leftover food. However, the amount of the products that can be stored at one time or for longer than a few days is limited by the small size of the refrigerators and by erratic power outages in winter.
Food preservation is widely practiced. Ninety five percent of women interviewed for the baseline in Jalalabad and 71 percent of those in Jumgal preserved food in 2014. Food preservation involves manipulating fresh products in order to stop ripening and slow or halt decomposition by bacteria, yeast, and molds. This is most often done by sealing off air, or by adding sugar, salt, or acid. This manipulation may also involve heating the product. The most common method of preservation, namely canning, consists of packing foods that have been sterilized by heat into jars and sealing out all air. Ideally, the jars are also sterilized prior to filling them, and the filled jars are further processed in boiling water or with steam pressure to kill anaerobic pathogens such as botulism. These last two steps, which are globally recommended, are not always practiced in Kyrgyzstan.
Produce most commonly preserved in all regions are cucumbers as pickles, and tomatoes. There are a lso varying versions of mixed vegetables, which are usually sautéed in oil before being sealed in jars. These are simply known as “salad” and present the most risk for botulism because they are low in acid. Soft fruits such as berries are made into jam. Other fruits, particularly apples, cherries, plums, and peaches are canned as “compote” which is a small amount of fruit with water and sugar added. In the case of fruits, whether preserved as jam or as compote, the long cooking time destroys virtually all the vitamin C content, which means they primarily contribute calories and some fiber to the winter diet. During field work, it was evident that rural women were very proud of their canning efforts and motivated to preserve food this way as much by an enjoyment of the flavors as by the need for a variety of food available in winter. From observations during the formative research, the amount of food canned or pickled is small for the size of the households.
The other method for preserving food, used primarily in the south, is solar drying. Eighteen percent of families interviewed for the baseline in Jalalabad had dried some food. This method is used for apricots, plums, and grapes. When asked, people had not heard of drying vegetables. It should be noted that the hot dry summers in the south are good for this type of food preservation. Much of the fruit that is dried is sold rather than saved for home consumption.
Other than tiny compartments in refrigerators, people in the target area do not have access to freezers. Freezing fruits and vegetables would preserve more nutrients, eliminate the need to add sugar or salt, remove the risk of anaerobic food borne illness, and be much more cost effective than canning, which requires expensive jars, lids, and heat.
Food Attributes
Women in the focus groups and in the food availability exercise were asked to name foods that are forbidden for, or not consumed by, different family members, including pregnant women and young children. In all regions, but particularly in Jumgal, women had received a message that the frozen chicken sold in markets and shops (usually imported from China) is full of hormones and dangerous to the health of everyone. They said they previously consumed more chicken until they learned this. It is unclear where the message originated, but it seems to have been widely disseminated in very recent years.
In lower Jalalabad, women said they wouldn’t use cottonseed oil, preferring oil made from other plants such as corn or soy. This may be because of their intimate knowledge of cotton-growing, including heavy use of pesticides on the crop.
There is also concern about the safety of eating purchased mayonnaise. No one could articulate what the safety issue might be, but a government decree banned it from being served in preschools and kindergartens. This issue has been around for quite some time.
Women have heard that liver is good for preventing and curing anemia, but they shy away from eating it because they have frequently seen liver flukes when butchering an animal. This is an animal health issue that could be addressed by agriculture programs.
The only foods that women identified as unacceptable for very small children were spicy foods made with peppers. They said that children wouldn’t like them. More investigation could be completed about foods deemed unacceptable for small children.
The theme of foods considered unacceptable for pregnant and lactating women needs to be further explored as nothing emerged in the discussion. This may have been because of the presence of health workers in the focus groups.
Food Consumption within the Household
Families reported that they eat two or three meals together per day. Some families prepare hot food only for the evening meal. Women are responsible for food preparation. They were asked during focus groups whether they eat while preparing food and all reported that they do, particularly raw vegetables such as carrots, cabbage, tomatoes, cucumbers, and onion. They also share these snacks with children who are present. Women also reported that they often eat while cleaning up after a meal, for example, finishing soup left by a child.
| Foods women consume between meals |
|---|
| Jumgal: bread, cookies, apples, wheat national drinks, corn drink, kefir |
| Jalalabad: bread, cookies, apples, dried or fresh apricots, kefir |
| Toktogul: bread, cookies, corn when in season, wheat drinks |
Women in the focus groups said they frequently eat between meals, often three or four times a day. This practice was much more common among women who do not work away from home. Snacks vary somewhat across the regions as shown in the box at the left. This non-meal food consumption may be a significant source of extra nutrients and calories for women.
When asked whether men are favored in intra-household food distribution, there was consensus that men get a larger serving, but are rarely served different foods than the rest of the family because of the mixed dishes. Women in focus groups commented that if men and boys need more to eat, they can fill up on bread.
Leftover main dishes from the previous day are frequently re-heated to give to men for breakfast. Women and children are more likely to eat porridge, bread and jam for breakfast, always with tea in all regions. Table 4 shows the usual meals eaten in different regions.
Table 4. Foods Most Often Prepared for Family Meals
| Meal | Foods prepared |
|---|---|
| Breakfast | All regions: milk, cream, tea with bread, tea with jam or sugar, leftovers from the night before (mostly for men), butter or homemade sary may, and sometimes porridge made of buckwheat or wheat |
| Lunch | Jumgal: fried potatoes, macaroni, eggs Jalalabad: milk with rice, pumpkin with milk Toktogul: rice or pasta with vegetables |
| Dinner | Jumgal: mostly soup but also pasta filled with meat or vegetables (manti, samsa) Jalalabad: rice soup with vegetables, rice pilaf, with meat at least once a week Toktogul: rice pilaf with or without meat, pasta filled with meat and vegetables |
Focus group participants said that many pregnant women eat more than three meals a day. Some said when they were pregnant, they ate four, five, or even six small meals. They get advice from health workers to eat more during pregnancy and to eat more fruits and vegetables.
Nutrition Knowledge
Women who participated in the formative research exercises understand that some foods are better or more nutritious than others. Very few women, however, know the relative nutrition content of different foods. This lack of knowledge included health workers. For the most part, they were unable to identify good food sources for different nutrients when presented with a range of food photos. They could say that fruits and vegetables “are good for the body”, or that “vitamins prevent diseases.” They knew that it is important to use iodized salt, and many were able to explain that iodine prevents goiter, but others said it is for “making children grow smarter.”
Only the men who are Village Health Committee (VHC) members had some concept of malnutrition and anemia and their consequences. Other men in the focus groups and interviews equated the word nutrition with food in general. Some expressed that animal source foods make people stronger and healthier.
Current Child Feeding Practices
Immediate Breastfeeding
The most revealing information about immediate breastfeeding came from the baseline survey results. Virtually all children are delivered in maternity centers and women stay there with their infants for approximately five days. The survey found that almost all children were put to the breast within a few hours of birth, however, 11 percent of infants in Jalalabad and seven percent in Jumgal were given a pre-lacteal, usually infant formula or sometimes sugary water. It seems probable that the decision to give the pre-lacteal is being made by maternity staff rather than by the mother and is in accordance with the existing protocol for low birth weight infants or for women who have had a caesarian section.
Exclusive Breastfeeding
According to the baseline survey, 99 percent of new mothers initiate breastfeeding, however infants start receiving other liquids at one month and gruel by three or four months of age. Only one-third of children ages 0-5 months in the survey were being given breast milk exclusively, which is much lower than the 56 percent reported in the DHS.
Table 5. Liquids consumed by children ages 0-5 months
| Liquids consumed by children ages 0-5 months SPRING baseline survey | Region | |||||
|---|---|---|---|---|---|---|
| Jumgal | Jalalabad | Total | ||||
| Count | % | Count | % | Count | % | |
| Breast milk | 67 | 85% | 99 | 99% | 166 | 93% |
| Plain water | 47 | 60% | 38 | 38% | 85 | 48% |
| Tea | 21 | 27% | 28 | 28% | 49 | 27% |
| Commercially produced infant formula | 12 | 15% | 15 | 15% | 27 | 15% |
| Milk such as tinned, powdered or animal milk | 6 | 8% | 13 | 13% | 19 | 11% |
| Any other liquids | 2 | 3% | 13 | 13% | 15 | 8% |
| Fortified, commercially available infant and young child food | 4 | 5% | 4 | 4% | 8 | 5% |
In the focus groups, women said they start giving other liquids because they think their young child must be thirsty. Many also said they are afraid they are not producing enough breast milk and some said they think infant formula is good for the child. Some said they have been told by health workers that breastfeeding is still considered exclusive if they are only giving other liquids, but not food, to their child. Table 5 highlights liquids consumed.
No one talked about breast problems interfering with breastfeeding. Women agreed that they don’t leave breastfeeding babies with caretakers except in real emergencies and then, they might leave formula or cow milk for the child. Using a bottle to feed the other liquids is common, even among children older than six months.
There is a general belief, particularly in Jumgal, that breast milk is not sufficient after two or three months, that the baby is hungry and therefore that it is necessary to start giving semi-solid food. This is usually a thin gruel described further below in the section on complementary feeding.
About a third of women in the focus groups say they still use a traditional cradle with swaddling. Babies are left in the cradle four to five hours at a time or overnight. It is unclear whether babies are lifted out for breastfeeding, and if not, what effect this might have on breast milk production.3
In general, breastfeeding is viewed as an important practice, and women receive support from their mothers-in-law and other family members to have time to breastfeed and to eat well while lactating. However, as shown in the baseline survey, women discontinue breastfeeding long before the recommended two years, with only about half of women still breastfeeding when the child is one year old. During focus groups, women said they quit when they become pregnant again or when they took a medicine, or when they had no more milk. A few women mentioned that the Quran says not to breastfeed when pregnant with another child, but eminent religious leaders say that this is not found in the Quran.
Complementary Feeding
In both target areas, but particularly in Jumgal, complementary feeding starts too early rather than too late. The baseline reported that fewer than 15 percent of children between the ages of 6 and 8 months were not getting food in addition to breast milk. By nine months, all children were being fed solid or semi-solid food.
The most common first food in both regions is a gruel called bulymak, which is made by browning flour in animal fat and adding either milk or water, and sometimes sugar. At first, it is made to be very thin, but as the child grows, the thickness of the gruel increases. Many women in the focus groups reported giving this food to their child daily while others said they made it every other day. Children are also given other porridges, mashed potatoes and rice as early foods. Many women also give sweet biscuits or bread.
Women in the focus groups said they feed their child at regular mealtimes and many give small children snacks as well. It appeared that many had not received messages about how often to feed their child and some who had heard the recommendation thought it meant preparing hot food more times a day, which they wouldn’t have time to do. Most women said children are given food on a separate plate.
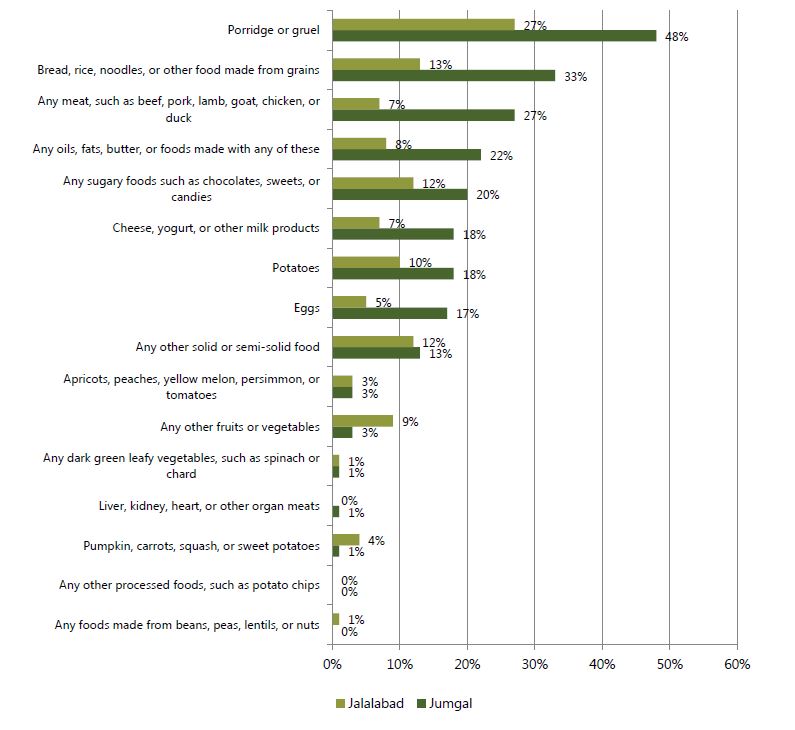
Table 6 lists the different foods children ate in the 24 hours prior to the baseline survey. Children ages 6-23 months in Jumgal ate a mean of 2.9 food groups out of seven, while in Jalalabad the mean was 3.3 food groups. The table shows that children in Jumgal were given more animal source foods while children in Jalalabad were given more vegetables, which is consistent with the focus group findings.
Table 6. Solid and semi-solid food consumption among children ages 0-5 months yesterday during the day or night
In general, women participating in focus groups did not appear to have received much information about optimal child feeding practices. They reported getting some advice from health workers, but tend to follow suggestions from their mothers or mothers-in-law to feed the child in traditional ways.
Water, Sanitation, Hygiene
Access to Clean Water
Access to clean, piped water in Jumgal is generally very high. Families go only a short distance to a public standpipe to retrieve water and some families have a standpipe in their yard. According to local leaders, approximately 5 percent of families have water piped into their homes. According to the baseline survey, few families in Jumgal treat their water, which may be acceptable since the water is coming from a protected source.

The situation is more complex in Jalalabad, as shown in the graph to the left, where many more people have access to water piped into their yard or dwelling, with approximately one quarter of households getting water from a public standpipe, and the rest getting surface water or water from an unprotected spring. The baseline survey reported 98 percent of families surveyed say they treat their water, usually by boiling. The concern is the 13 percent of families that use surface water, which is often contaminated by agro-chemicals or mining waste in this zone. During the formative research, boys were observed drinking from a drainage channel along a street as well as from an irrigation ditch.
Latrine and Toilet Coverage and Condition
The 2012 DHS reports that 99 percent of all households and 94 percent of rural households have a ventilated improved latrine or a latrine with a slab. This definition of slab did not specify material. The 2014 Multiple Indicator Cluster Survey (MICS) reports that 97.5 percent of all households have access to an improved toilet facility, with no definition given for “improved.” The SPRING baseline also considered any latrine with a slab as improved, but the translation of the word “slab” in Kyrgyz specifies that the slab has to be cement/concrete, not wood or other material. With this more specific definition, 90 percent of households in Jumgal and 31 percent in Jalalabad use unimproved latrines. The formative study used observation to verify this and also observed for the presence of latrines at public institutions (schools, health facilities, eating establishments, etc.) and the hygienic conditions of the toilet facilities. Observations are highlighted in Annex G.
Researcher observations revealed that many or most latrines are in poor condition, and roofs and doors are sometimes missing. Some were located quite close to houses, but most were a reasonable distance away. No handwashing facilities were observed close to household latrines. Most importantly, the latrines observed were unclean, with excrement all around the hole. Virtually all latrines observed in Jumgal and many in Jalalabad have a wooden “slab” which is considered an “improved latrine” by international definition, but these are harder to clean than cement and subject to rotting away quickly.
Not all health facilities have latrines. The ones that had latrines kept them only slightly cleaner than household latrines. Toilets inside hospitals and maternity centers were reasonably clean although some lacked running water, hence, were pour-flushed. Water and soap were available for handwashing at health facilities.
The situation at schools is concerning. All of those observed had some kind of latrine and usually had separate sides for boys and girls, but there was often just one of each for a school with many students, and all of them could be described as filthy. In two cases where donors had constructed very nice latrines of sufficient number for both boys and girls, these new facilities were locked up and unused. Only these new latrines had handwashing stations.
If anything, latrines observed in other establishments including a restaurant, city hall, office buildings, and business establishments were the least hygienic of all. It was evident that anyone who enters one will subsequently track fecal matter outside upon leaving, which has serious health implications. While very small children may not go near latrines, the pathogens are brought right to their play areas.
Since the formative research team could not find clean household latrines in order to conduct a Doer/Non-doer study of the barriers and motivators to maintaining clean latrines, the study relied on interviews with school personnel and VHCs, using a tactic of having them analyze the reasons why other people in their communities don’t use latrines properly and keep them clean. To assess potential for sanitation marketing, the study team also asked random individuals in Jumgal about interest in, and barriers to, indoor plumbing as well as why the few households who have indoor toilets keep them clean.
It is evident both from observations and discussions that the prevailing social norm is unclean latrines. There is no felt need to keep them clean, no sense of disgust or shame because everyone’s latrine is in the same unhygienic state. Other barriers cited by the VHCs include the lack of running water near homes, the lack of cleaning materials, and laziness. On the other hand, there was agreement that the incentive to keep indoor toilets clean is to prevent or eliminate odors. Obviously, anyone who has an indoor toilet also has piped water which makes cleaning easier.
When asked, individuals cited that the principal reason they might want, or have, an indoor toilet is for the benefit of an elderly or disabled household member. No one mentioned other benefits of indoor plumbing such as not having to go out into the cold or for the convenience of small children. For most households in Jumgal, cost is the major barrier to an indoor toilet, because they would not only have to pay for plumbing the house but also for putting piped water into the house from the nearest source and building a septic tank.
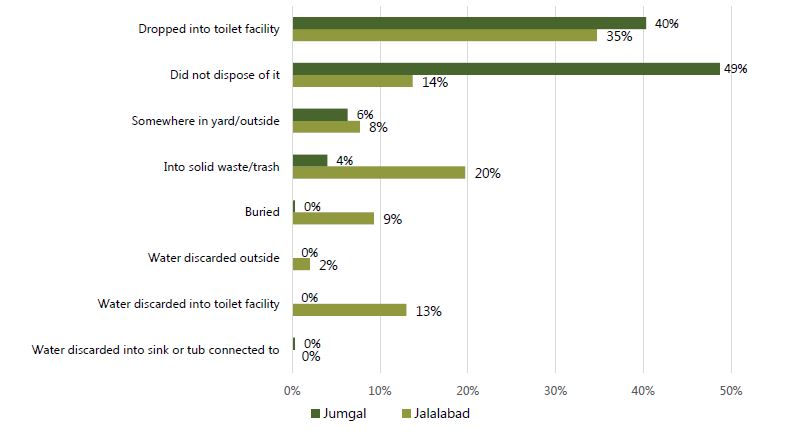
The results of the baseline survey reveal a problem with proper disposal of children’s feces. More than half of women in both Jumgal and Jalalabad did not dispose of their children’s feces properly by putting them in the latrine or toilet. Table 7 below shows that feces are often simply left outside the house or put in the trash. The formative research did not investigate attitudes about children’s feces or why they are not put in the toilet or latrine, therefore, this will have to be included in another round of research.
Table 7. Location of child feces disposal last time child passed stools
Other Environmental Hygiene Issues
The study team observed additional aspects of environmental hygiene as well. In smaller villages, garbage disposal was a very evident problem. Household garbage is tossed into vacant lots or left along the side of the street. One of these dump sites of waste from a market area was adjacent to the Jumgal District Hospital complex. Domestic animals scavenge in the garbage while children play nearby.
In observing for conditions that are associated with environmental enteropathy, such as children’s contact with animal feces, the team noted that chickens roam freely around dooryards. Other livestock are kept in pens farther from the house, but manure may be tracked on shoes to the house, although shoes are always removed before entering the house. Women appeared quite conscious of what children were putting in their mouths and children are generally set down on rugs, not directly on the ground. Therefore, we concluded that exposure to environmental enteropathy pathogens is not high, except in summer when small children may play outdoors without direct supervision.
Handwashing
According to the baseline survey, most women reported that they wash their hands after going to the toilet, before eating, and before preparing food, but less than half wash their hands before feeding a child and very few wash their hand after toileting a child. This last action provides further evidence of the belief that children’s feces are harmless.
Further investigation is recommended to learn about barriers to handwashing at all appropriate times. It seems from the good coverage data that access to water should not be a barrier. The baseline also reported that the vast majority of families have soap for hands at the place of washing but over a quarter of women admitted they don’t always use soap when washing their hands.
Gender and Intra-Familial Dynamics
In modern Kyrgyzstan, gender and women’s roles show the influence of not only traditional Kyrgyz pastoral culture, but also the centuries of living in mixed communities with Russians, and the Soviet influence on education for women and working women. According to the DHS and the SPRING baseline, 99 percent of women have at least a high school education. In Jumgal, 46 percent have post-secondary training or education, while in Jalalabad, 35 percent of women interviewed have post-secondary training or education. The baseline found that about one quarter of women interviewed work in some profession, a relatively high percentage considering that most of the target area is rural with few available job opportunities.
The formative research found distinctions between Jumgal and Upper Jalalabad with Lower Jalalabad in terms of women’s roles in agricultural work. In Lower Jalalabad, women report working long hours in their family fields or for other farms, especially during planting and harvest seasons. In the other two areas, where agriculture is primarily livestock-raising, women reported spending little or no time on agricultural activities other than caring for poultry and livestock kept near the house such as a milk cow.
In all areas, caring for vegetable garden is primarily the responsibility of women, with men taking an active role in preparing the soil and harvesting. Decisions about what to plant and sell are often made jointly, but women report that they usually decide by themselves or with other women in the household. Decisions about selling large livestock are usually made exclusively by men, who are also responsible for care of the large animals.
Housework is considered the domain of women, however, fetching water was observed to be almost entirely the responsibility of young boys. Except in some very conservative families, women have independence in mobility. In focus groups, men reported that it is up to a woman to decide whether to seek health care for herself or a sick child, but in most families, she would have to discuss it with her husband because she would need to ask him for money. Men feel it is their role to handle family finances.
Some newly married couples live with his parents until they can afford a house of their own. The mother-in-law has primary decision-making responsibility about what foods to purchase and prepare, although she may expect the young woman to complete food preparation. Older women also influence child care decisions within the house, as noted above in the discussion of child feeding practices.
Among those of Kyrgyz ethnicity, young men must pay a bride price, either in cash or livestock. In return, the young woman’s family must provide a dowry of a household start-up package, which will include furniture, kitchen utensils and bedding, and may include appliances such as a stove or small washing machine. Thus, the number of assets a young couple has may be a reflection of her parents’ affluence or the size of bride price they received rather than a measure of wealth of the young couple itself.
Health Facility Assessment Results

The purpose of the HFAs was to obtain an overview of conditions and of supplies available at health facilities, particularly items related to providing nutrition-related services. The HFA was conducted using a checklist for observation and reviewing patient records. Whichever health worker was available to show the researcher around was also given a brief written exam consisting of seven questions to assess practical knowledge. The tools used for the HFA can be found in Annex C. The SPRING staff member in charge of this part of the research, a physician, has many years of experience conducting similar assessments and monitoring health facilities throughout Kyrgyzstan.
In total, this assessment included 23 health facilities of all sizes. These included five maternity centers, six Family Medical Centers (the main referral centers for a district), and eight lower level centers called Family Group Practice and two rural health posts called FAPs. The sample was purposive; these medical facilities were located in or adjacent to the sites selected for other formative research activities.
The health facilities visited had most necessary equipment along with growth charts. All of the health facilities had some kind of toilet facility, but 9 of the 23 were rated as being in very poor condition. Six of the health facilities in the HFA did not have running water inside, and five others did not have a functioning handwashing station. Almost all of them had the handwashing protocol displayed and soap was available, even if there was not water on hand. While the observation guide did not document this, several of the health facilities did not have central heat, while others had coal stoves in one room and still others had only small electric heaters in some rooms.
None of the health facilities had handout materials on any nutrition topics nor audio visual equipment. Several had nutrition-related posters on the wall, but some were outdated and others were not adapted to the Kyrgyzstan context. Only two health facilities had the existing anemia treatment protocol for pregnant women and five had the protocol for anemia in children. None of the health facilities had iron supplements available to distribute free of charge. Only the Jumgal health facilities had Gulyzak (a micronutrient powder) fully stocked and available for distribution (provided by the Swiss Red Cross.)
The review of clinical records for pregnant women revealed that they are neither being prescribed iron supplements according to the protocol, nor is there the recommended follow up for those who are told they should purchase iron. More details are provided in a separate formative research report on anemia.
In general, there are deficits in record-keeping, although records are much better kept in Jalalabad than in Jumgal. Of particular note was one Family Medical Center that had no records for children under age two. Additional investigation will be needed to identify the barriers to keeping complete and accurate records. The results of the HFA are shown in the chart in Annex H. More detailed descriptions are available in Russian for staff use upon request.
An additional component of the HFA consisted of giving a short training needs assessment to one or more available professional staff at each facility. This short exam existed of seven practical questions as shown in Annex C. The exam was administered to 67 health workers including 42 nurses, 6 gynecologists, 4 feldshers (medics), and 5 family doctors. The average score was 2.17 out of 7 points possible, and gynecologists and doctors did not score better than nurses or feldshers. All tested had difficulty with the two questions related to prevention of anemia and counseling on the side effects of taking iron supplements. A surprising number of the respondents could not explain counseling messages for pregnant women nor explain the purpose of using iodized salt. They all scored relatively better on recommendations for breastfeeding and complementary feeding.
Recommendations
- Implement IYCF, BFHI, and anemia training, as stated in the project work plan, for all health workers in the target areas. Follow up with supportive supervision and mentoring to ensure institutionalization of protocols, and new skill development.
- Conduct supportive supervision jointly with district health officials, with particular attention to improving charting/record keeping.
- Collaborate with local governments and district health officials to ensure that each health facility has a clean, functional latrine and that the number of latrines or toilets is appropriate for the number of staff and patients.
- Work with local governments and district health officials to provide handwashing stations and a consistent supply of clean water.
- Ensure that the Strategic Behavior Communication strategy includes ample nutrition materials for distribution or display at health facilities.
- Assist the Ministry of Health to develop a new anemia protocol, including designing a training for health workers on implementing the protocol, and a system for distributing iron–folic acid, which has already been procured along with MNP (Gulyzak) for Jalalabad.
Footnotes
1 The Kyrgyz Republic Demographic and Health Survey, 2012, was conducted by the Kyrgyz National Statistical Committee, the Ministry of Health, and the USAID MEASURE project. The sample included 8,208 women of reproductive age and 2,636 women with children under age five. Fieldwork was conducted in August through December of 2012.
2 http://documents.wfp.org/stellent/groups/public/documents/ena/wfp262003.pdf Accessed 11/19/14
3 This question specifically asked whether a mother lifts the infant out of the cradle to hold him/her while breastfeeding or whether the mother simply leans over the cradle to breastfeed.