
Prior to the recent Ebola virus disease (EVD) outbreak, Sierra Leone faced nutritional challenges, with 76 percent of its children anemic and 29 percent stunted (SLMN 2013; SMART Survey 2014). The findings from the 2010 and 2014 SMART surveys, conducted prior to the Ebola outbreak, indicated that Sierra Leone was on a trajectory to reach the World Health Assembly target of reducing stunting by 40 percent, lowering the incidence of stunting to 20 percent by 2025. District level data is not as positive, and in the two areas covered by this report, Bombali and Tonkolili, the same surveys show increases in stunting from 28 to 33 percent and from 33 to 41 percent, respectively. Moreover, the 2014 data was collected from June-August, just as the outbreak was beginning to unfold. The outbreak prevented data collection activities in two areas and potentially skewed the national results of the surveys (SMART Survey 2010; SMART Survey 2014). With EVD confirmed in the country in May, food security and nutrition impacts likely intensified in July 2014, when the Government of Sierra Leone (GoSL) began enforcing quarantines and restricting movement to control the spread of EVD.
As part of USAID’s Ebola recovery efforts, USAID/Sierra Leone and USAID/Washington’s Bureau for Food Security (BFS) requested that the SPRING conduct a nutrition assessment in Bombali and Tonkolili districts. As per guidance from USAID/Sierra Leone, Tonkolili District was the focus of fieldwork. The objectives of the assessment were to—
- identify contributors to undernutrition, including social and behavioral constraints on nutrition;
- document effects of the EVD outbreak on food, agriculture, health, and nutrition services and systems; and,
- determine best approaches for improving nutritional status during the first 1,000 days.
The following report summarizes the findings of the nutrition assessment conducted between August and October 2015. SPRING first conducted a desk review of 48 documents followed by a two-week field assessment, collecting information from a total of 242 key informants and group discussants. The assessment was undertaken by a cross-disciplinary group of nutrition, social behavioral change, and agriculture experts. SPRING’s rapid qualitative assessment confirmed many themes from the team’s desk review and results were consistent with more in-depth studies and population-based surveys. Furthermore, discussions with government representatives, community members, and implementing organizations revealed many common challenges and opportunities related to nutrition, health, agriculture, and behavior change communication.
Overall, SPRING found the current situation in Sierra Leone is one of low agricultural production, poor health, limited availability and access to vegetables and animal-source food, and poor understanding of the contributors to or consequences of poor nutrition. EVD had a large impact on current agriculture and health services and our findings confirmed the need for substantial new investments in Sierra Leone. Given the dire situation, there are many approaches that can be used to address the problem. But these need to be carefully thought through and highly targeted given the current situation. Based on the findings of this needs assessment several recommendations were identified. Some of the key recommendations include—
- continue to promote a multi-sectoral approach across government institutions and other stakeholders to ensure nutrition remains a high priority
- design, test, and scale-up a nutrition-specific and nutrition-sensitive social and behavior change communication strategy that complements existing materials and builds demand for more diverse diets comprising more nutrient-rich foods
- implement community-based interventions to increase availability, access, and consumption of nutrient-rich foods, such as increasing diversity and productivity of community and household farming systems, including but not limited to vegetable gardens, fishponds, and raising small ruminants and poultry
- support the establishment of a functional health system to implement direct nutrition and infection interventions
- ensure that nutrition-specific and nutrition-sensitive agriculture interventions achieve optimal nutrition outcomes through synergistic goal-setting and shared geographic and beneficiary targeting
- promote a range of interventions that strengthen the role of women in agriculture to increase their control of income while empowering them and their husbands to recognize the importance of saving time and labor for their own nutritional well-being and that of their children.
Assessment Objectives and Methodology
Objectives
The purpose of this nutrition assessment is to provide USAID/Sierra Leone with a background and further understanding of the program context for nutrition in Sierra Leone. It is hoped that this information will inform the development of USAID’s investment and implementation plan in the district of Tonkolili. The specific objectives of the assessment are to—
- identify the key contributors to undernutrition, including the type and extent of social and behavioral constraints on nutrition, especially those of dietary diversity and protein consumption among children and pregnant/lactating women
- document the effects of the Ebola virus outbreak on food, agriculture, health, and nutrition services and systems that need to be considered relative to future programming
- apply assessment findings to determine best approaches for improving nutritional status, especially of pregnant and lactating women and children under two years of age.
Methodology
USAID/Sierra Leone and USAID/Washington’s Bureau of Food Security requested the assistance of SPRING to conduct a thorough nutrition assessment in Bombali and Tonkolili Districts——the proposed zone of influence (ZOI) for Ebola recovery funding under the Feed the Future Initiative——and to advise the Mission on the way forward for addressing nutrition using an integrated and systematic approach. Based on guidance from USAID/Sierra Leone, much greater attention was given to fieldwork in Tonkolili District——a focus that SPRING fully agrees with given the high levels of stunting, wasting, and underweight among children under five years of age and women of reproductive age. To better understand the current nutrition situation, the SPRING project first conducted a desk review examining more than 48 policy and program documents, published articles, notes from relevant in-country meetings, and quantitative population surveys. The field assessment was conducted from September 16 to October 2, 2015 by a team of nutrition and agriculture experts and local research assistants. The team’s daily schedule can be found in Annex 1.
Semi-structured key informant interviews and group discussions were conducted using guides developed for adaptation to Sierra Leone’s context, covering a range of parameters associated with both direct and underlying contributors to nutrition. National and district level data collection was conducted in English and community-level data collection was conducted primarily in Temne and supplemented with Krio. Interview guides were written in English and the district data collection team agreed upon standardized language in Krio during a one-day training. The tools were pretested in Bombali Sheborain Bombali, half a mile from the Tonkolili border. The fieldwork was undertaken by a team of six researchers, including four Sierra Leoneans (one female, three male).
A total of 242 informants provided information via key informant interviews and focus groups with government staff, local and international NGOs, and community members (farmer-based organizations (FBOs), agricultural business centers (ABCs), mother support groups, women’s groups, and market venders). These meetings provided insight into the current nutrition-related programming and challenges across Sierra Leone and within the ZOI. The communities were selected by the Ministry of Agriculture, Forestry and Food Security (MAFF) extension unit and NGOs (Concern International, Action for Community Transformation and Sponsorship, and International Medical Corps). In addition, the assessment team visited local markets and informally met with market sellers. At the end of each day, the team convened to review discussions and findings. These daily meetings allowed the team members to address commonalities, differences, and important areas to focus on as they moved forward with fieldwork.
Table 1. SPRING Meetings in-Country
| District | Chiefdom | Meetings | # |
|---|---|---|---|
| Western Area | Freetown | ACF, BBC Media Action, Concern, FAO, Focus 1000, HC3, HKI, IFAD, IMC, IITA, IrishAid, JSI, MAFFS, MOHS, National Federation of Farmers in Sierra Leone, Save the Children, SUN committee, Sierra Leone Chamber for Agribusiness Development, Sierra Leone Seed Certification Agency, UNICEF, WorldFish | 43 |
| Tonkolili | Magburaka | ACTS, IMC, MAFSS, MOHS | 147 |
| Konike Barina | LANN women’s group, community leaders | ||
| Kunike | LANN women’s group, community members | ||
| Kalifa Rowala | Mother Support Group, health workers, community members | ||
| Kafe Simira | Mother Care Group, animator, health worker, community members | ||
| Kolifa | ABC, community members | ||
| Bombali | Makeni | ACDI/VOCA, WFP MAFFS, MOHS-DHMT, World Hope, BRAC, Caritas, SLARI | 52 |
| Bombali Shebora | Community leaders, community members | ||
| Total | 242 | ||
Country Background
Sierra Leone has four regions comprising 14 districts; Northern: Bombali, Kambia, Koinadugu, Port Loko, and Tonkolili districts; Eastern: Kailahun, Kenema, and Kono districts; Southern: Bo, Bonthe, Moyamba, and Pujehun districts; and Western: Western Area Urban and Western Area Rural (AED 2009). Though rich in resources, Sierra Leone is one of the world’s poorest countries, with over half the population living below the poverty line (CIA Continually updated; UNDP 2015a; WB 2015a). Five military coups since its 1961 independence and an 11-year civil war (1991-2002) have devastated social, economic, and physical infrastructure (AED 2009). Sierra Leone has held two democratically organized elections since the war, but the residual effect of the war and the persistent high rate of unemployment remain potentially destabilizing factors (Freedom House 2012; openDemocracy 2015).
Sierra Leone ranks nearly last (183 out of 187 countries) in the 2014 Human Development Index (HDI) with high youth unemployment/underemployment (estimated at 70 percent) and adult literacy at only 41 percent (UNDP 2015a; UNDP 2015b). The mean household size is 5.9 members, 46 percent of the population is under age 15, and 42 percent of households have children who are orphaned or living with neither their mothers nor fathers (DHS 2014).
Since May 2014, Sierra Leone has been plagued by over 8,704 cases of Ebola virus disease (EVD), taking the lives of nearly 3,600 people. As of October 2015, the country is still working toward resilient zero, or the 42 days of no cases required to declare Sierra Leone Ebola-free (NERC 2015). The Government of Sierra Leone (GoSL) has restricted movement, through curfews, lockdowns, quarantines, and school and selected market closures, to curb the epidemic (Poraj-Wilczynski 2015). The outbreak has also been linked to a continued decline in household food security and health service use (acaps 2015b). Ebola has disrupted livelihoods, employment opportunities, and agricultural production (WFP 2015a). GoSL restrictions aimed at controlling the EVD crisis discouraged many farmers from working in their fields and many households struggled to find laborers for their farms (WHH, FAO, MAFFS 2014). Schools closed for nine months, during which children experienced increases in child labor and exploitation, exposure to violence in the home and community, and teenage pregnancy (Risso-Gill and Finnegan 2015).
Before EVD struck, forecasts for 2014 had estimated a 12 percent growth in real GDP. However, with the onslaught of EVD and low international market prices of iron ore, on which Sierra Leone is highly dependent, the real GDP growth in 2014 was 7 percent and its 2015 GDP is forecasted to contract by as much as 24 percent (WB 2015b). Agriculture—largely based on cacao beans and coffee for export—comprises the largest share of GDP (62 percent) (WB 2015a; FAO/WFP 2014). Though milled rice production makes up 85 percent of all cereal production and rice is grown on 88 percent of all cereal cropped land, production is still insufficient to meet demand. Rice still makes up the majority of all agricultural imports (FAO/WFP 2014). Two-thirds of the population engages in subsistence agriculture (FAO/WFP 2014).
Nutrition Situation
The findings from SPRING’s nutrition assessment for Sierra Leone are organized to reflect a combination of information gathered from secondary sources as well as from key informants and group discussants who helped the assessment team members to understand both direct and underlying contributors to undernutrition, especially in the target districts of Bombali and Tonkolili. Key informants in Freetown helped the team to better understand the enabling environment for nutrition nationally, as well as to become familiar with the range of investments from both the GoSL and other donors.
Nutritional Status
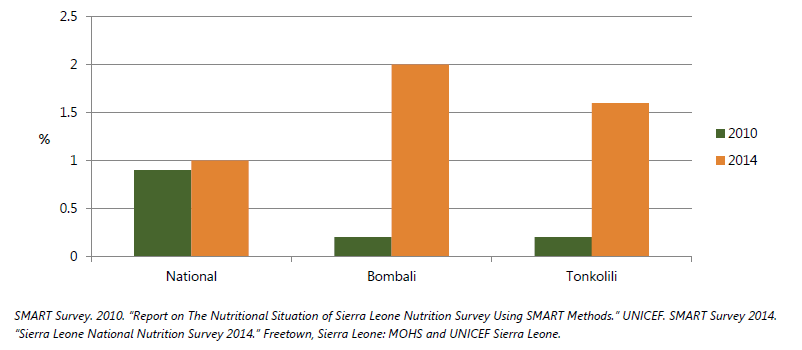
Based on Standard Monitoring and Assessment of Relief and Transitions (SMART) surveys conducted in 2010 and 2014, chronic malnutrition decreased nationally by 5 percentage points. However, all key nutrition indicators have gotten worse in both Bombali and Tonkolili districts, reflecting a serious problem, even before the effects of EVD (figure 1). And, per figure 2, below, severe acute malnutrition is of high public health concern (SMART Survey 2010; SMART Survey 2014). UNICEF is undertaking a nutrition survey with results expected in November 2015 to provide a picture of whether these numbers have worsened since the EVD outbreak.
Figure 1. Nutrition Status among Children 6-59 months, Stunting and Underweight
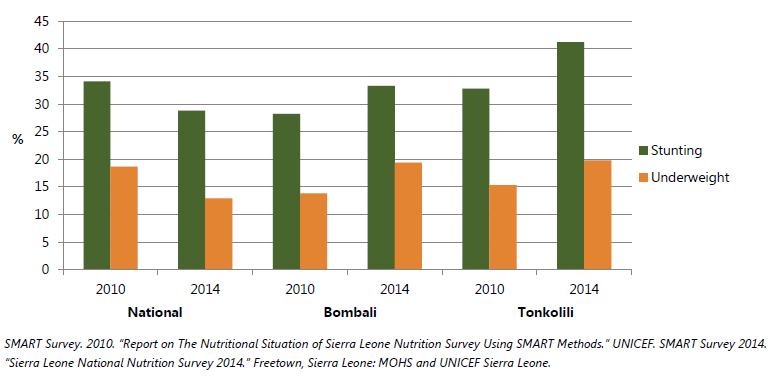
Figure 2. Nutrition Status among Children 6-59 months, Severe Acute Malnutrition
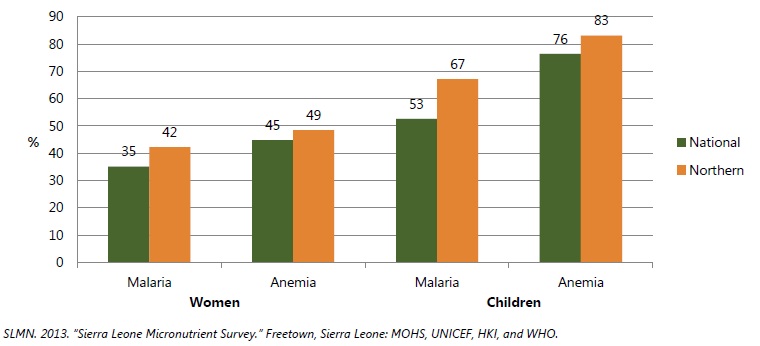
Sierra Leone’s anemia prevalence is among the highest in the world. Forty-five percent of non-pregnant women, 70 percent of pregnant women, and 76 percent of children 6 to 59 months are anemic, with figures slightly higher in the north. Globally, iron deficiency is generally assumed to account for approximately 50 percent of anemia, but in Sierra Leone, iron deficiency appears to be very low (8 percent of women and 5 percent of children). This data is surprising and warrants additional investigation, given the low intake of animal source foods, the high intake of phytates, and the higher prevalence of iron deficiency in select neighboring countries. Vitamin A deficiency is high among children (28 percent), but almost non-existent among women (2 percent) and may contribute to childhood anemia, although the mechanisms of the relationship between anemia and vitamin A deficiency are still not well understood.
The prevalence of inflammation is extremely high in Sierra Leone with more than 70 percent of children having elevated levels related to malaria, helminth, diarrheal disease, and lower respiratory infections. The prevalence of malaria is of particular concern and the regions with the highest prevalence of anemia also have the highest prevalence of malaria (SLMN 2013). See figure 3.
Figure 3. Malaria and Anemia among Women Aged 15–49 and Children 6-59 months
During the national micronutrient survey, mothers reported that thirty percent of children had diarrhea in the two weeks preceding and 10 percent had a lower respiratory infection (SLMN 2013). Another survey found respiratory infection to be as high as 26 percent in Bombali (SMART Survey 2014). In addition, other parasites, including soil-transmitted helminthes, are endemic and only 58 percent of children 12-59 months are dewormed (SPRING 2014; SLMN 2013). The generally low prevalence of micronutrient deficiency and the high prevalence of infections and inflammation indicate the latter may be a more important driver of anemia.
The high prevalence of stunting and anemia is a manifestation of the vicious cycle between malnutrition and infection. Inadequate nutrition impairs immunity, increases the risk of infection, and, in turn, creates greater nutritional requirements consequent to the infection. Therefore, nutrition is both a risk factor and an outcome of infection. Furthermore, without addressing infections individuals will not be biologically responsive to food-based interventions.
Water, Sanitation, and Hygiene
With high parasite prevalence and low levels of preventative treatment, poor water, sanitation, and hygiene (WASH) are especially problematic (table 2). About 66 percent of households nationally—76 percent in Bombali, and 35 percent in Tonkolili—have access to “safe” water (SLMN 2013). But only 39 percent of water points can be used year-round due to rain or dry conditions (acaps 2015c). Tonkolili has some of the most overused water points and, therefore, one of the greatest deficits of potable water in the dry season (acaps 2015c; Fongar 2014). In Bombali, the main improved water source is a borehole (44 percent) or a protected shallow well (29 percent), but in Tonkolili, over half of households (61 percent) obtain their water from a river or stream. In both districts, the majority of surveyed households (86 percent) do not treat their water (SLMN 2013). Additionally, only 20 percent of schools have access to clean water and only 4 percent of schools in Tonkolili and 3 percent in Bombali have functioning latrines (acaps 2015c). Per SPRING’s field assessment, awareness and, in some cases, infrastructure for water, sanitation, and hygiene (WASH) exist, but consistent and widespread use of key WASH practices is lacking. The EVD outbreak further limited access to water as maintenance of water points and movement of water delivery trucks and water purification supplies were interrupted. It also delayed WASH development activities and concentrated WASH activities at facilities at the expense of the wider community.
Only 38 percent of households have access to improved sanitation. In Bombali 6 percent and in Tonkolili 33 percent of households report defecating in the open (SLMN 2013). The rainy season brings problems of runoff from land surfaces into the water supply (ODI 2014). Nevertheless, households interviewed in the needs assessment reported having a latrine in their compound, but acknowledged practicing open defecation when away from the home (especially while at their farms and traveling to and from the farms). While key informants reported appropriate handling of food and child feces, national surveys indicate that in both Bombali and Tonkolili, hand-washing after handling child feces and before cooking is extremely uncommon (SLMN 2013). Surveys conducted prior to the EVD crisis indicate that less than one-third of households in both districts have a place most often used for hand washing, and soap and water at hand washing stations was essentially non-existent (DHS 2014). On the positive side, respondents from the needs assessment reported substantial increased hand washing sensitization, possibly due to government soap use campaigns since the EVD crisis. According to health care respondents, the most recent campaign occurred in March 2015 and each household received a bar of soap. Since the EVD outbreak, responses from key informants indicate a dramatic improvement in hand washing. Concerted efforts need to be made to ensure these new habits are maintained.
Table 2. Key Water, Sanitation, and Hygiene Conditions Contributing to Malnutrition
| National 2013 | Bombali 2014 | Tonkolili 2014 | |
|---|---|---|---|
| Households w/access to safe water | 75 | 76 | 35 |
| Households that treat water effectively | 14 | 9 | 4 |
| Households with soap at the location for handwashing | 49 | NA | NA |
| Households w/access to improved sanitation | 38 | NA | NA |
Diet and Feeding Practices
Diet Quantity and Quality
SPRING found the total amount of food consumed by households to be inadequate. Key informants report that a family of 5-10 people will eat, on average, five ties of leafy greens, two fish, and 12 cups of rice per day, while others reported as little as two cups a day for a family of 6. While three rice-based meals are considered satisfying, many households usually prepare only one substantial meal each day and the leftover food is often covered and kept overnight for breakfast. Snack consumption of pepper cakes, groundnuts, and seasonal fruits does occur but is infrequent. Wild food items are consumed on a regular basis and also sold to earn income. These include krain-krain (a wild green also cultivated close to homes), yams, young oil palm fronds, palm oil, palm kernel oil, plum, and malombo (a wild green fruit). Processed foods are rarely consumed.
Rice is the primary stable food in Sierra Leone followed by cassava. Households in Tonkolili and Bombali reported that a diet typically consists of rice with sauce made from palm oil, seafood, and potato, cassava, or krain-krain leaves (see Annex 2 for a full list of foods consumed). Other than fish, the amount and variety of animal products consumed is very low. A cross-sectional baseline survey for the LANN project in Koya chiefdom in Kenema plus Kunike and Kunike-Barina chiefdom in Tonkolili found fish consumption to be high (92 percent) (Fongar 2014). But, while all respondents reported eating fish regularly, SPRING determined that fish was usually added in small quantities to sauce to provide flavor, indicating that fish consumption is unlikely to be a large source of protein and micronutrients in many households. While 89 percent of households own an animal, they rarely consume animal source foods (meat 7 percent, eggs 1 percent, and milk products 1 percent). Livestock (mainly goats and sheep) and poultry were reportedly used primarily as a source of income and so are eaten only on special occasions. Prior to the EVD crisis, many families supplemented their diet with bush meat, but during the EVD crisis this practice was curtailed. However, SPRING found that hunting and consuming certain types of bush meat continues, despite the ban.
Data from population-based surveys in Sierra Leone classify household dietary diversity scores (HDDS) in the medium range with a score of 4.6 nationally, 4 in Bombali, and 4.1 in Tonkolili. Individual dietary diversity scores are similar to household scores with non-pregnant and pregnant women reporting having eaten 4-6 food groups in the previous 24 hours. Young children’s food diversity scores are much lower, however, reflecting poor infant and young child feeding practices (Fongar 2014).
Mandatory fortification of vegetable oil with vitamin A and of wheat flour with iron, zinc, vitamin D, and B vitamins are planned as part of Fortify West Africa, an initiative supported by the U.S. Government and other donors. But consumption of these products varies, with 49 percent of all households (mostly in urban and western areas) and only 9 percent of the poorest households using commercially-produced vegetable oil. Wheat flour is consumed less among the poor and iodized salt has relatively low coverage in the north (SLMN 2013). To serve the communities in the ZOI, other strategies besides commercial fortification would be required.
While the Sierra Leonean diet is not completely devoid of micronutrients (with fish, leaves, groundnuts, and fruits offering sustenance), significant improvement in the intake of quality foods is needed. Cooking methods to reduce bitter tastes and hard-to-chew greens result in over-cooking and loss of vitamin content. In addition to low consumption of animal based foods, respondents repeatedly mentioned a limited surplus and demand for vegetables.
Findings related to the distribution of food within the household were mixed. Sometimes family members eat together and other times food is set-aside for the husband to eat when he returns home. In larger families the women and girls often eat from different bowls than the boys and men. Alternatively, sometimes the women and children eat from the same bowl. In general, children are the first to consume leftover food for breakfast, followed by the husband, while the wife will only eat if there is any remaining food. Many informants reported that men receive the highest quality and greatest quantity of food. Reasons frequently cited were that men perform more physical labor and thus require additional food to “stay strong” and that feeding the husband well was also viewed as a wife's “expression of love.” A study supported these findings and also found that boys received greater portions than girls based on the belief that boys perform more physically demanding activities. In addition, that study found mothers-in-law receive preferential consideration in the distribution of food, based on the belief that in-laws have earned such meals (ODI 2014).
The needs assessment revealed several food taboos for pregnant women and young children and these foods tended to be the most nutritious and beneficial foods. Consumption of chicken, eggs, and fish were the most common foods reported to cause physical harm; e.g., There is a belief that fish or eggs consumed by a pregnant woman will cause her child to become a thief. The government and NGOs reported actively undertaking behavior change communication activities to overcome various taboos. Nevertheless, some respondents still reported these practices being followed. See tables 4.1 and 4.2 in Annex 4 for a list of foods one should purportedly avoid in Sierra Leone during certain periods of the lifecycle and the rationale.
Infant and Young Child Feeding Practices
Infant and young child feeding practices (IYCF) in Sierra Leone are generally inadequate (table 3). While respondents answered in the affirmative when asked if they exclusively breastfed, upon further probing they reported providing water, mashed up bananas or plantains, and cassava for the baby to suck. Two mother leaders both (independently) recognized that the most difficult behaviors to change among the group members are child feeding habits. One specifically noted the challenge of prohibiting children under six months from chewing on a boiled cassava, not as nourishment but as a relatively clean distraction/object to handle, suck and play with. During the early stages of the EVD crisis, mixed messages were disseminated on the safety of breastfeeding. A harmonized message on breastfeeding is now being spread (Box 1). Figures provided by UNICEF show a cumulative of 695 children required replacement feeding. Importantly, all key informants did not perceive EVD and related-messaging influencing breastfeeding practices within the general public.
Table 3. Key Infant and Young Child Feeding Factors Contributing to Malnutrition
| National 2013 | North 2013 | Bombali 2014 | Tonkolili 2014 | |
|---|---|---|---|---|
| Breastfeeding within one hour of delivery | 66 | 64 | 54 | 59 |
| Exclusive breastfeeding until six months | 42 | 42 | 63 | 61 |
| Complementary feeding (children 6–8 mo.) | 42 | 40 | NA | NA |
| Minimum frequency of feeds (children 6-23 mo) | 26 | NA | 5 | 16 |
| Minimum dietary diversity (children 6-23 mo) | 35 | 30 | 34 | 29 |
| Minimum acceptable diet (children 6-23 mo) | 13 | NA | NA | NA |
Competing demands on women’s time likely contribute to poor self and infant and young child feeding. Women typically return to their farm work 2-4 weeks after delivery, leaving the infant at home to be cared for by others, often for long periods of time. Respondents reported not wanting the children to starve or cry and so provide infants with water or food while their mothers are away. Some mothers reported telling their mothers-in-law not to provide food while they are not at home and reported expressing breastmilk into a clean cup. Health care providers and NGOs highlighted mothers’ workload as the most significant barrier to exclusive breastfeeding. While not addressed in this needs assessment, a study found one barrier to continued breastfeeding is a widespread belief that a couple should not have intercourse during the months when a child is breastfeeding (ODI 2014).
Furthermore, a recent survey, which covered portions of Tonkolili, indicated that meat was given to only 2 percent of children 6-24 months and dairy products to only 4 percent (Fongar 2014). Many respondents reported appropriate complementary feeding, such as “soft rice with lots of sauce” and providing homemade “Bennimix,” consisting of sesame, fish, and maggie/salt/sugar. However, upon further probing, it became apparent that children often receive the general family diet, as well as biscuits dissolved in hot water, powdered milk, and sugar. Rarely (once a month), a boiled egg may be fed to the child. Ripe banana, cooked yam with palm oil on top, guava, mango, and pineapple are also given to children between 6-23 months. A less expensive alternative to this recipe is corn flour, sugar, and water, which will make enough food for two days and costs 1000 leones. Children over 24 months eat the same food as adults and are served first when meals and quantities are limited. They receive proportionally more sauce on their rice than adults. While reportedly fed 3-4 times a day by some, less affluent households prepare meals once in the evening, and leftovers are consumed in the morning. School feeding programs provided children with an extra meal, but these have been suspended due to EVD and have not been reestablished.
Box 1: Breastfeeding and Ebola*
- Mother's suspected of having EVD should cease breastfeeding and only resume if they are found to be EVD free.
- Children of mother's with EVD are provided breastmilk substitutes until six months of age and then introduced to complementary foods.
The most frequent reasons respondents gave for providing inappropriate complementary feeding were the time and costs associated with making specific foods for young children. Lack of maternal control in household decision-making may also account for the poor diet of children. In this needs assessment mothers often described themselves as the primary decision makers on breastfeeding their children. However, many women mentioned the husband decides when a child will first receive solid foods. Furthermore, a recent IYCF barrier analysis found husbands, grandmothers, and mothers-in-law exert significant influence on a mother’s exclusive breastfeeding. Relatives frequently encouraged mothers to provide water, rice porridge, and formula (HKI 2015). In terms of self-care of pregnant and lactating women, the SPRING team heard many women indicate that they eat well during pregnancy and become choosier about what they eat. Lactating women claimed to eat more than usual and that they rest for 2-4 weeks after delivery, then they return to the fields.
Health Services
Sierra Leone has 50 private and GoSL hospitals and similar facilities/providers and 1,092 peripheral health units (PHUs), staffed by 300 government (and some private) maternal and child health (MCH) aides. GoSL health care offers 211 doctors and dentists (9 doctors per 100,000 people), 655 nurses of different classifications, 122 public health officials, and eight each of pharmacists and laboratory technologists. There are also 13 nutritionists (two national, two in hospitals, and nine with District Health Management Teams). Health personnel are most heavily concentrated in the west (MOHS 2012). There is a deficit of adequately trained and supervised community level workers and existing workers lack salaries, supplies, and an information system to work with. Community Health Worker (CHW) guidelines are currently being revised, which makes it challenging for implementing NGOs to use them as a platform for nutrition programming.
According to District Health Management Team (DHMT) staff, there were 208 PHUs in Tonkolili and Bombali at the time of this assessment. SPRING learned that there is a performance-based finance system in place, with each PHU receiving funding quarterly according to the number of immunizations, deliveries, and antenatal care (ANC)/post-natal visits conducted. On the nutrition front, since 2014 there has been a rapid scale-up of outpatient therapeutic feeding (OPT) programs and approximately 50 percent of PHUs provide OPT. The results of mid upper arm circumference (MUAC) screenings in the summer of 2015 prompted funding from WFP to implement an additional 3-month supplementary feeding program (SFP) that will conclude in October 2015. Only one location in Tonkolili, the district hospital, handles children with severe acute malnutrition (SAM) with complications. While UNICEF will continue supporting the SAM center, district health officials recognize the need to continue the moderately acute malnutrition (MAM) supplementary feeding centers after October.
Quality of health services is often poor, with studies showing inadequate water supply during the dry season (acaps 2015c), inconsistent electricity at health facilities (Fofanah 2015), and lack of general supplies (only 35 percent of facilities have the basic equipment required for service delivery) (Fofanah 2015). Stock-outs reported to the SPRING team result in only 28 percent of 14 essential medicines being available where needed (GoSL 2015). Health information systems generally do not inform decision-making, given the lack of timeliness and poor quality of data. The SPRING team learned that surveillance reporting provided by PHUs to the district health office includes: number of children who have been screened for MUAC, including those with MAM or SAM; early initiation of breastfeeding; exclusive breastfeeding for six months; low birth weight; babies weighed within 24 hours of birth; vitamin A supplementation to children and postpartum women.1 But problematically, in SPRING’s review of surveillance documents, there seems to be substantial misreporting by PHUs. District health officials reported a need to improve PHU reporting and monitoring capabilities, so that the data might be correct and more useful for analyses.
Access to health services in rural Sierra Leone is a challenge on several levels. SPRING heard that clinics are often far from homes (up to nine miles away), with long waits. In general, use of health services drops during the rainy season (May-October) due to poor road conditions. During the dry season, when more people are apt to seek services, water supplies at clinics are lower. Though many women in the needs assessment reported seeking ANC, the number of visits rarely met the recommended 4-visits per pregnancy. Women reported often not being able to receive basic components of the ANC package, including antimalarials and IFA tablets, and are inconsistently provided counselling. This finding is supported by quantitative studies; for example, few women received IFA in the north during their last pregnancy and only 28 percent of women took 90 tablets (SPRING 2014). The SPRING team heard that while there is a modest fine of 5,000 Leones for home delivery, and incentives for traditional healers and birth attendants (TBAs) to bring women to health facilities for delivery, some women still give birth at home. SPRING also heard from communities that health care workers may charge fees for services that, under the Free Care Act, are supposed to be free of charge (e.g., those for PLW and children under five) (GoSL 2015). This often restricts access to care given that many households are not in a position to pay for services or for the indirect costs of care-seeking (MOHS 2011c).
Outreach activities are limited and SPRING heard that while district nurses and nutritionists may conduct mobile outreach activities, low budgets and lack of transportation result in TBAs being important providers of health care (ODI 2014). To supplement the deficit of formal service providers and to better reach communities, the GoSL is establishing Mother Support Groups (MSGs) throughout the country. These MSGs include the SNAP Mother Care Groups, the national NGO, ACTS, support of MSGs in all 11 chiefdoms of Tonkolili, and World Hope’s smaller-scale effort with MSGs in Bombali. In some cases, the field agents supporting the MSGs are often unable to visit and support the MSGs. Without sufficient training and support, these groups could actually compound the problem of ineffective use of information. This is complicated by low literacy levels among Mother Leaders.
Impact of EVD
At the height of the EVD outbreak, only 4 percent of PHUs were closed (Fofanah 2015). However, SPRING heard from health officials in Tonoklili that during the EVD crisis, communities were afraid to use health services and the Ebola Needs Analysis Project reported that while 80 percent of the population typically seeks health care, during an outbreak, only 50 percent did (acaps 2015a). Nationally, there was a 90 percent drop in family planning visits (Fofanah 2015); women attending four ANC sessions dropped 14 percent; and institutional deliveries dropped 7 percent. Bombali had the greatest declines, with 25 percent and 19 percent respectively (UNICEF 2015). Use of child health services also declined, with Penta3 vaccinations dropping 17 percent in October and January 2014/15 compared to the same period in 2013/14 (Fofanah 2015; UNICEF 2013). Of particular concern for nutrition, there was a 28 percent reduction in the number of children attending growth monitoring and promotion. District level staff reported growth monitoring and promotion was stopped to prevent contamination during the EVD crisis in response to a case where an affected child’s height and weight were taken.
13 | Sierra Leone Needs Assessment Except in the heavily affected districts, including Bombali, the majority of facilities are now open and being used, though still less than before the outbreak (acaps 2015a). Women giving birth in a clinic increased from November 2014 (28 percent) to May 2015 (64 percent), and those receiving at least one antenatal care visit increased from 56 percent to 71 percent in that same period (Mayhew 2015). The EVD outbreak seems to have supported improvements in WASH generally, with health staff maintaining positive behaviors and encouraging communities to be involved; for example, in screening for SAM (e.g., measuring MUAC), reporting deaths, safe burials, and maintaining sanitation practices. For example, health staff now use gloves when they touch patients and have recently revised weighing protocols so they are using large plastic bowls cleaned with bleach after each weighing.
Food Security
Household food security is strongly linked to the agricultural cycle (SMART Survey 2014), per figure 4 below (FEWS NET 2013). The rainy season starts in April and the lean season follows soon after, lasting for 2-3 months, until the harvest of the rice crop, which is supposed to carry the household through the land preparation season. In 2014, approximately one-third of the rice consumed during the dry season was household-cultivated, but only 6 percent of rice cultivators can rely on their own production to meet their family’s rice needs throughout the year (SMART Survey 2014; CFSVA 2011). By and large, incomes come from sales of crops and livestock (85 percent), followed by small trades/businesses (6 percent), and others (4 percent) such as mining, transportation (bike transportation/”okadas”), fishing, teaching, and carpentry (SMART Survey 2014). Consequently, food insecurity increases sharply during the June-August lean season, when about 45 percent of the population is food insecure (CFSVA 2011). Table 4 below highlights levels of food security in Bombali and Tonkolili.
Figure 4. Food Security by Agriculture Cycle
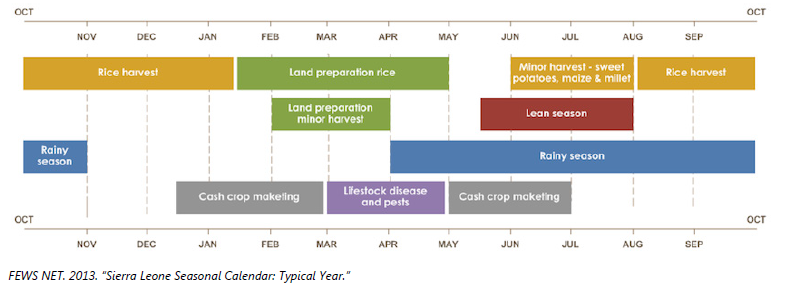
Table 4. Food Insecurity in Zone of Influence
| District | Bombali | Tonkolili |
|---|---|---|
| Total population | 518,909 | 392,997 |
| % of HHs* severely food insecure | 2% | 23% |
| Population severely food insecure | 10,897 | 88,424 |
| % of HHs moderately food insecure | 23% | 52% |
| Population moderately food insecure | 121,425 | 202,786 |
| % of HHs food insecure (severe + moderate) | 26% | 74% |
| Total population food insecure | 132,322 | 291,211 |
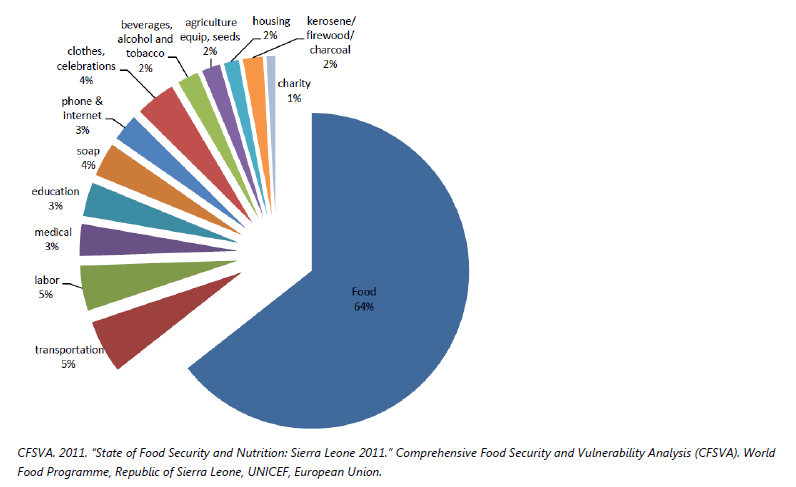
In the June-August period, in Bombali and Tonkolili, the vast majority of households obtain most of their food through purchase (81 percent of households in Bombali and 74 percent in Tonkolili). About 20 percent of households spend over 65 percent of their income on food, with another 40 percent spending 50-65 percent of their income on food (SMART Survey 2014; WFP 2015a). The WFP’s Comprehensive Food Security and Vulnerability Analysis (CFSVA), completed in 2011, reflects the range of household expenditures as a percentage of total income, as seen in figure 5.
Figure 5. Household Expenditure
Rural households rely on a range of livelihood activities for year-round survival. However, those who rely primarily on food crop production tend to be most food insecure as measured by total food consumption (figure 6, below).
It should be noted that while households who relied primarily on income earned from mining employment tended to be more food secure—66.4 percent of mining households consume an acceptable amount of food (calories)—findings from SPRING’s fieldwork indicate that EVD is likely to have longer-term negative effects on the mining communities due to the departure of mining companies and loss of both incomes and farm lands due to reductions in mining operations. Figure 7 below shows levels of food insecurity by livelihood.
Figure 6. Food Insecurity in Zone of Influence
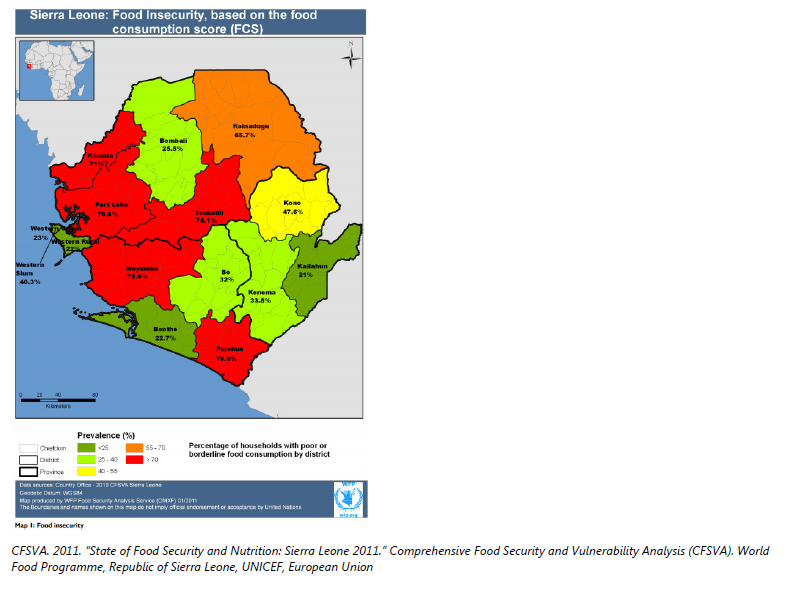
Figure 7. Food Insecurity by Livelihood

At the national-level, over half of household heads indicated employing food coping strategies. The most common strategies included relying on less preferred foods (69 percent), kinship support or borrowing (61 percent), reducing portion size (43 percent), reducing the number of meals (40 percent), and restricting adult food consumption (24 percent) (SMART Survey 2014). Another study found that households diversify their livelihood activities—for example, fishing and selling fish—in order to buy food until the harvest comes in (ODI 2014).
The SPRING assessment team learned from respondents that staple foods produced by the household last only 6-8 months of the year and this can be attributed to low productivity associated with the predominant upland production farming system, post-harvest losses, and sometimes households being forced to sell produce immediately after harvest to repay loans made during the planting season. The SPRING assessment team also found all respondents reporting use of at least one coping mechanism during the lean season. Key coping strategies mentioned by respondents during the SPRING assessment included—
- reduce the number, portion, and quality of meals consumed (mainly for adults)
- cultivate indigenous vegetables, such as eggplant and krain-krain
- prematurely harvest domestic and wild food
- gather and barter/sell wild foods, including palm kernels
- sell local rice and purchase imported cheap rice of lesser quality
- sell chickens, eggs, goats and sheep
- hunt and consume and/or sell bush meat
- borrow from neighbor, from lenders or savings group
- cash/other donations from relatives.
The timing of the EVD outbreak had a significant effect on rice production, which decreased by 39 percent over the previous year’s harvest (WFP 2015a). An Emergency Food Security Assessment found that as of April 2015, 95 percent of key informants said the food situation was worse than at the same time the previous year, due to decreased production, increased prices, movement restrictions, and trade disruptions. Other food security-related issues reported by respondents and supported by outside sources (FAO/WFP 2014; WFP 2015b; WFP 2015a; Peter Davis 2015) included—
- abandonment of farms that were then destroyed/infested by pests
- inability to hire farm labor
- reduced ability to sell or trade cash crops and other produce
- disruption of school-feeding programs
- limited access to bush meat due to regulations against hunting and consuming bush meat
- rise in food prices as produce became scarce
- families impeded from borrowing from kin living in other communities
- stoppage of value-added/”luma” market activities.
Figure 8. Traders Reporting Reduced Market Supplies of Main Commodities, July 2015
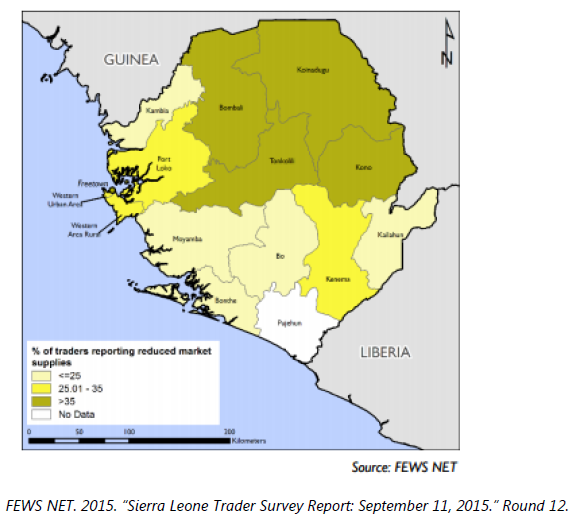
Figure 8 shows the percentage of traders reporting reduced market supplies of key commodities as of July 2015, with both Bombali and Tonkolili showing over 35 percent of traders having reduced market supplies. However, as the EVD crisis has been waning, respondents said the majority of the negative impacts listed above are no longer affecting their communities (with the exception of bush meat still being banned and the closure of markets on Sundays).
Women’s Empowerment and Gender Issues
As in most other West African countries, women in Sierra Leone play a large role in both agriculture and in the well-being of their families. SPRING found women’s traditional roles include post-harvest grain processing, storage, food preparation, fishing (mainly approaching the dry season), vegetable gardening, and raising poultry. Men, meanwhile, traditionally perform more energy demanding tasks, such as the initial clearing of the bush, burning shrubs when dry, initial tilling of the land, and rice threshing. Both men and women do secondary tilling, weeding, and harvesting. They also transport the harvest to town and raise goats and sheep. Children participate in all farming operations.
Per SPRING’s field assessment, despite shared responsibilities on and off the farm, women often consult with their husbands about how much of the household production to sell. The profits women make from their main agricultural or non-agricultural activities are usually shown to their husbands or, less frequently, the women give the profits to their husbands. Traditional roles also dictate that husbands decide when the family seeks health care, although in some households, wives consult/seek advice from their husbands and they decide together.
Married rural women do not own land, but have access to land for growing crops. Generally, women are poorly represented in decision-making regarding land, credit, household budget allocation, use of productive resources and the sale of farm produce, although this varies among households. Nonetheless, women carry the heaviest burden of household responsibilities, including the care and feeding of household members. MAFFS and the GoSL have recognized the important contributions of women in agricultural and economic development. As such, MAFFS created a “women in agriculture” unit under the Crops Division within MAFFS. The unit has a nutritionist who also has an office at the Food and Agriculture Organization of the United Nations (FAO) in Sierra Leone. The unit has programs on vegetable gardening, including how to properly prepare vegetables for consumption. While gender and women’s empowerment requires much more than a division office, women are slowly being elected to leadership positions in FBOs and related private sector organizations, such as the National Federation of Farmers in Sierra Leone, the largest farmer organization in the country.
Agriculture
Food Production

In Sierra Leone agriculture is the engine of economic growth, with 70 percent of the population in the target districts engaged in some form of agriculture for their livelihood. Agriculture—including crops, forestry, fishing, and hunting—accounted for more than half of GDP in 2014, a contribution that has been declining over time (50.5 percent in 2014 down from 58.2 percent in 2009), indicating a structural shift toward mining/quarrying (20.2 percent in 2014 up from 3 percent in 2009) (OECD 2015). As the primary livelihood in the likely ZOI, agriculture provides food that is consumed directly by rural producers and is the main source of income for purchasing both food and non-food items and services.
Smallholders, with an average 0.5-2 hectares of land, account for up to 70 percent of agricultural output, involving two-thirds of the farming population (AED 2009). Tonkolili and Bombali districts primarily grow upland and lowland rice and cassava. Other crops are maize, sorghum, millet, sweet potatoes, groundnuts, vegetables (such as okra, eggplant, tomato, leafy greens, onions, cucumbers, and carrots), and fruits (including pineapple, banana, mango, papaya, and avocado). Rice, cassava, beans, pumpkin, and potato are available all year, although the prices vary depending on the season. Main livestock include poultry, goats, and sheep. Livestock-raising was hampered by theft during the civil war and, therefore, food crops are the main source of income for the majority of households.

As in other parts of the country, farmers in Tonkolili District grow their food crops mostly in upland areas characterized by low soil fertility and depend entirely on rainfall. In order to mitigate risks associated with upland farming, the majority of smallholders practice “mixed farming,” which involves mixing rice seeds with small quantities of sorghum, maize, sesame, beans, and pigeon pea seeds. They also plant cassava at random. This farming practice results in low yields of all of the various crops grown with the rice. At the same time, leaving the harvested rice in the field results in post-harvest losses (see photo above). However, mixed farming also ensures that farming families will have something to eat regardless of climate shocks, including pest or disease infestation, weeds, and periodic droughts.
The lowland areas, including the inland valley swamps (IVS) and bolilands that have been developed for irrigation, are the agro-ecologies with the highest potential for maximizing food production, since they possess silty loam soils and are naturally flooded with fresh water from the rivers during the rainy season. In addition, these areas are made fertile by top soil eroded from the adjacent uplands. However, these areas are underutilized mostly due to the high cost of initial development, including for small-scale full irrigation. Individual farmers find it difficult and strenuous to clear the land and prepare the mostly clay soil. It is these two production areas (especially the IVS) that the MAFFS has targeted for developing small-scale irrigation schemes (10-50 ha) and for rehabilitating old schemes for rice production. MAFFS is therefore encouraging farmers to make more use of the lowlands and to place less emphasis on the uplands because of their low productivity.
Crops grown in irrigated paddy fields give the best yields globally, as irrigation provides possibilities for growing a variety of crops and 2-3 crop seasons per year, thus enhancing productivity. There is also the possibility of integrating crops/fish/livestock in the same area, which could bring about complementarities, such as the rice crop benefiting from the fish and animal droppings. The animals, in turn, feed on the crop residues, including vegetables. The enhanced productivity would result in an increase in food availability, which, in turn, may help to reduce or maintain more affordable prices for all. A reduction in prices for key staples, such as rice, results in increased purchasing power, even for the poor. This revenue could allow the poor to purchase additional, more nutrient-dense foods, provided they are aware of the value of consuming a diverse and nutritious diet.
Table 5, below, shows national rice area, production, average yields, and self-sufficiency, which demonstrate the low crop productivity highlighted in the preceding paragraphs. Although the GoSL has spent enormous resources on the rice staple food crop, yields have not only stagnated, they are quite low—less than 2 mt/ha. Increased production has been due to area expansion—from 258,850 ha in 2001 to 671,422 ha in 2013. The low yields can be attributed partly to the predominantly rainfall-dependent upland farming, where the soils are quite low in fertility. At the same time, farmers use limited (or no) modern agricultural inputs, such as improved seed and fertilizer. Maize yields (See note at the bottom of table 5), exceeding 2 tons/ha, are a bit better than rice. It is because of the low use of fertilizer by most of the West African states that the Economic Community of West African States (ECOWAS) recommended that member states endeavor to apply a minimum of 50 kg/ha to show their commitment to the CAADP framework for restoring agricultural growth. The USAID’s Feed the Future is closely aligned to the CAADP framework. Table 5 also shows that Sierra Leone has achieved over 100% self-sufficiency in rice production in 2013. However, the country continues to import large quantities of cheap low quality rice, including 100 percent broken rice.
Table 5. Sierra Leone National Average Rice Areas, Production, and Yields for 2001-2013
| Year | Area (Ha) | Production (Mt) | Yield (mt/ha) | Self-sufficiency (%) |
|---|---|---|---|---|
| 2001 | 258,850 | 310,620 | 1.20 | 37.93 |
| 2006 | 422,556 | 562,000 | 1.33 | 62.15 |
| 2013 | 671,422 | 1,255,559 | 1.87 | 119.93 |
*Note for comparison: maize yields in 2011 and 2013 were 1.52 and 2.10 mt/ha respectively
Poultry are commonly raised by women and are found in nearly all households in the target district. However, farmers rarely eat poultry or eggs, except on special occasions, because the animals provide a good income, some of which they use to purchase fish that is cheaper and generally available in the villages in dried or smoked form. Both men and women raise small ruminants (goats and sheep). These animals are generally left to find grass for themselves, especially during the dry season. The goats and sheep are generally kept in pens/small huts, but the chickens are often kept in jute bags or baskets at night and kept in the living rooms of houses, a practice that contributes to high rates of inflammation and illness, especially among young children. During interviews, SPRING learned that the lack of veterinary services and supplies for the animals were major constraints to expanding production.
Eighty-four percent of households have a home garden and vegetables are grown for direct consumption and for sale (81 percent of households sell some portion of their garden crops). Growing fruits is also common and 71 percent of households growing fruit use it for both consumption and sale (SMART Survey 2014). The selection of vegetables and fruits grown is driven by several factors, including availability of seed, perceived market demand, and land area availability. Nutritional value is not generally considered. Nearly all households reported collecting and consuming wild foods, but aside from krain-krain and amaranth, there was limited evidence of these in the markets. Needs assessment respondents consistently reported not having the resources (e.g. seeds and other inputs) to grow different types of nutritious foods as a major challenge to small farm families.
During SPRING’s visits to farms, farmers reported grain losses during storage and processing. According to the farmers, approximately 30 percent of harvests are lost due to grain spoilage (e.g. if the grain is left for too long in the field after harvest) and pest (rats, birds, wild animals, and insects) and disease infestation. Post-harvest losses are also due largely to lack of appropriate storage facilities, such as community grain stores (e.g. the ABCs constructed by MAFF). Concern International is implementing a project to address grain storage losses due to rats, but the larger problems of post-harvest management have not yet been addressed.
Agricultural extension and services
The extension service is one of six divisions within MAFFS. The other five divisions are crops, livestock, engineering, forestry, and monitoring and evaluation. The same administrative set-up is found at the district level. The extension service is responsible for disseminating technologies developed by the Sierra Leone Agricultural Research Institute (SLARI) to farmers, helping organize farmers into FBOs, and conducting training programs. Some of the training is done jointly with SLARI, especially on the use of new and promoted technologies. Agricultural information is also passed on to farmers through radio broadcasts, which are aired approximately twice per month. The engineering division develops new irrigation schemes and rehabilitates old ones. The division also supervises irrigation-engineering work contracted out by MAFFS.
A “women in agriculture unit” is located in the crops division and has a nutritionist who assists with programs such as vegetable gardening (including preparation and consumption). The programs are also coordinated with the extension service. NGOs implementing food security programs (e.g. Concern Worldwide) also provide extension services to establish vegetable gardens.
The introduction and promotion of FBOs and ABCs in 2008 – 2010 was a result of efforts by MAFFS, FAO, the United Nations Development Programme (UNDP), and NGOs to support the Farmer Field Schools (FFSs) extension methodology. Upon graduation from the FFS, 2-3 groups of FBOs are encouraged to come together to operate an ABC for the purpose of starting an agribusiness. Over 150 ABCs have been established by MAFFS’s jointly with FAO. SPRING visited a typical ABC in Tonkolili and interviewed several group members at the collective and the household level. SPRING’s main finding from these conversations is that, while the concept and objectives for the approach are good, both the ABCs and FBOs have serious management and technical constraints that have rendered them unable to fulfill their important mission of increasing yields and incomes of farmer members. Table 6 below shows the numbers of FBOs, ABCs, and extension agents in Bombali and Tonkolili.
Table 6. Number of FBOs, ABCs, and Extension Agents in Bombali and Tonkolili
| District | # FBOs | # ABCs | # Extension Agents | # ABC Members | |
|---|---|---|---|---|---|
| Male | Female | ||||
| Bombali | 162 | 18 | 30 | ||
| Tonkolili | 203 | 35 | 40 | 4023 | 2762 |

As is true in many countries in West Africa, most GoSL agriculture extension agents lack transportation to get to the field. While this challenge can be demotivating, low compensation and lack of opportunities for training also tend to discourage even the most dedicated agents. Agricultural schools provide little opportunity for students to obtain field experience, so they have to rely on the farmers themselves to obtain experience. Recognizing this problem, MAFFS is currently working with the Njala University to revise its curriculum to be more field-oriented, so that students graduate with greater confidence in their ability to help farmers solve practical problems. This planned curriculum also supports the creation of National Dietary Guidelines, and mass media communication is planned to deliver social and behavior change communication (SBCC) nutrition messaging. As a part of the National Dietary Guidelines, a recipe book was created in partnership with FAO and will be incorporated along with the guidelines into training for MAFFS extension workers, providing an opportunity to ensure that the curriculum is nutrition-sensitive.
Agricultural Inputs
The unavailability and lack of access to agricultural inputs, especially fertilizers and seeds, were identified as major constraints to improving food security. This lack of access to seeds includes for the vegetables used in the emerging women’s gardens initiated by both NGOs and the community.
Table 7 shows the amount of fertilizers imported by MAFFS, its projects, and a select number of private input companies from 2010 to 2014.
Table 7. Quantities (MT) of Fertilizer Imported by MAFFS, its Projects, and Input Wholesalers
| Fertilizer Type | 2010 | 2011 | 2012 | 2013 | 2014 | Total |
|---|---|---|---|---|---|---|
| 15-15-15 | 217 | 275 | 442 | 491 | 600 | 2,025 |
| Urea | 205 | 200 | 623 | 285 | 300 | 1,613 |
| 18-46-0 (DAP) | 10 | 200 | 168 | 100 | - | 478 |

MAFFS sells fertilizer at a subsidized price of Le110,000 per 50kg bag (about $22.00) to anyone who buys it at its stores when available. Agro-dealers buy the fertilizer from MAFFS stores and transport it for sale with prices varying from Le150,000 – Le250,000, a heavy cost to farmers, many of whom cannot afford to purchase these inputs. This dependence on the government subsidy often results in limited amounts of inventory within agro-dealer shops. For example, during SPRING’s visit, there was no fertilizer at MAFFS stores in Bombali or Tonkolili. The government supplies all agricultural inputs from fertilizers, to seeds, to equipment, despite policy reforms aimed at privatizing the various sectors, including the agricultural inputs sub-sector. As a result, only a limited number of private agricultural input wholesalers have emerged, but a greater number of agro-dealers/retailers exist (see Annex 4, table 4.3).
In the case of seeds for field crops, SLARI provides breeder and foundation seed, while certified seed is produced by MAFFS’s Seed Multiplication Program using contract farmers, including FBOs. FBOs also receive foundation seed to produce certified seed. With the exception of vegetable seeds, improved seed for field crops is composite (seeds can be used for two or more years without renewal), not hybrid seed developed by commercial seed companies. The horticulture station of SLARI at Kabala in Koinadugu district is screening and trying to produce seed of local vegetables consumed in the country. According to SLARI, they have collected up to 50 local vegetables that are now consumed in the country and found to have comparable nutritional value to those imported.
Effects of EVD on Agricultural Prices, Incomes, and Services
During the initial EVD period, food prices were reported to have risen substantially, particularly when there were weekend lock-downs. Most people would rush to buy as much as they could afford to ensure that they had enough to eat. Many farmers were afraid to go to the farms to work, so production decreased. The EVD onset coincided with the planting season, and by rice harvest time, it had affected the entire country. In addition, the closing of all “luma weekly markets” and Sunday closing of local markets contributed to increased food prices affecting households of the lowest wealth quintile most. Since September 2014, increasing food availability has stabilized prices.
The restrictions imposed on movement of people affected practically all services and activities, including extension agents, since travel permits were needed to travel within and between districts. With many of these travel restrictions since lifted, MAFFS agents and other (private or NGO) service providers should be able to reach farmers and production groups, provided that transportation challenges are overcome.
Enabling Environment
If the environment is not strong or supportive of program design and implementation, investments to improve food, health, and/or care may not be effective in improving nutrition. In this assessment report we explore three elements identified in the literature (EngenderHealth 2011; Perez-Escamilla et al. 2012; Gillespie et al. 2013) as critical for an enabling environment – policies; governance and management; and resources (see Box 2).
Policies
The Republic of Sierra Leone joined the Scaling Up Nutrition (SUN) movement in January 2012. At that time, Sierra Leone had developed a number of policies and designed programs and strategies including the Free Health Care Initiative and the Sustainable Agricultural Development Program (SUN 2015). The policies most critical to nutrition are summarized below:
- The National Food and Nutrition Security Policy (NFNSP), developed in 2012 and led by the Ministry of Health and Sanitation (MOHS), emphasizes several key strategies: 1) use of the Essential Nutrition Actions (ENAs) framework to coordinate nutrition messaging; 2) nutrition and food surveillance and early warning, including use of Community-based Management of Acute Malnutrition (CMAM), Community-Based Integrated Management of Childhood Illness (C-IMCI), and nutritional care for those with HIV and tuberculosis; and, 3) prevention of nutrition-related diseases, especially through supplementation, fortification, deworming, promoting consumption of locally available micronutrient-rich foods, and access to potable water and sanitation (MOHS 2012).
- The Food and Nutrition Security Policy Implementation Plan (FNSPIP) was developed in collaboration with all relevant sectors and launched in 2013 (GoSL 2012b). The FNSPIP has a strong multi-sectoral focus and is aligned with the other sector policies, such as, the National Health Sector Strategic Plan 2010-2015 (GoSL 2012a); the Reproductive Newborn and Child Health Policy (MOHS 2011b); the Reproductive Newborn and Child Health Strategic Plan 2012-2015 (MOHS 2011c); the Free Health Care Initiative (GoSL 2009b); the National Malaria Control Strategic Plan 2011-2015 (MOHS 2011a); and the National Strategic Plan HIV/AIDS 2011-2015 (GoSL 2002).
According to the FNSPIP, MAFFS will support a number of nutrition-sensitive household food security activities including the integration of nutrition messaging into agriculture extension, collaboration with the private sector to improve processing and storage, training community members on processing and preservation technologies, promoting diversified household food production, and encouraging sustainable income generation for women (GoSL 2012b).
This emphasis on nutrition is not consistent with the MAFFS policy 2009 National Sustainable Agriculture Development Plan (NSADP), which promotes small-holder value chain development (GoSL 2009a). Apart from the NSADP, in 2010 the MAFFS mandated food fortification standards for flour, salt, and oil.
- Sierra Leone‘s Third Generation Poverty Reduction Strategy Paper (2013 – 2018) – the “Agenda for Prosperity” – was finalized. This strategy aims to position Sierra Leone as a middle income country and places a high priority on nutrition, articulating eight strategies for the health sector to reduce infant, under-five and maternal mortality through nutrition services and calling on other sectors to engage in nutrition-specific and -sensitive interventions (GoSL 2013).
- The National Dietary Guidelines are in development and Sierra Leone’s regulation to respond to the Code of Marketing of Breastmilk Substitutes. The Ebola outbreak may have temporarily interrupted some of this work, but the goals remain the same, and MOHS wishes to revitalize these efforts.
- The National Ebola Recovery Strategy for Sierra Leone 2015 – 2017 emphasizes the revamping of the agriculture and aquaculture sectors as well as ensuring access to nutrition services for severely malnourished children. In this strategy, the GoSL vows to restart livelihoods and to support the food value chains so that families can access viable alternatives to bush meat. Nutrition-sensitive interventions in agriculture (such as training agricultural extension workers in nutrition), social protection, and education sectors are also included (GoSL 2015).
Governance, Management, and Accountability
The FNSPIP serves as a common framework for coordinating ministries, local government actors, and development partners in scaling up nutrition activities. Nonetheless, coordination is a challenging task. The National Food and Nutrition Security Policy calls on several ministries to support improved nutrition and the FNSPIP provides step-by-step guidance for coordination between the MOHS and the MAFFS, among other entities (MOHS 2012; GoSL 2012b). However, just 1.8 percent of the total proposed budget has been allocated to date for coordination of nutrition programs (GoSL 2012b).
- The civil society consortiums in Freetown have been strong, particularly in response to the EVD crisis. In Tonkolili District, a civil society food working group has been created. However, the GoSL has expressed concern about these consortiums working independently of government efforts and has asked that they not be created or maintained. The MOHS views the formation of a multi-sectoral anemia working group as a priority and has requested support to form one within the SUN movement. In Tonkolili District, a Food and Nutrition Forum was established in response to EVD recovery efforts. It includes representatives from the MOHS, MAFFS, the Ministry of Education, and NGOs. District council meetings are held monthly, but focus on reporting rather than collaboration.
Capacity and Financial Resources
For management of the FNSPIP, the MoHS and Ministry of Finance and Economic Development (MFED) staff have been trained on tracking and financing nutrition activities (SUN 2015). However, little has been done to identify a nutrition champion within the government or to build leadership capacity. The total cost of the FNSPIP over five years is estimated at US$117.2 million, an average per capita annual cost of just over US$3.30. A substantial five-year funding gap of $81 million is estimated (SUN 2013). According to the SUN movement, “the Government has shown commitment and pays wages salaries and utility costs as outlined in the implementation plan. However, disbursement remains a challenge. Financial contributions are made by donors for some nutrition direct and sensitive interventions (SUN 2015).”
Summary of Key Challenges
A full description of the key findings that resulted from this desk review and data collected in the field are described in detail above. This section provides a synopsis of the issues frequently and consistently identified during the desk review and key informant interviews as the main challenges at the national and district-levels, with a specific focus on the Tonkolili district:
- Despite increased theoretical understanding of the importance of linking nutrition to agriculture, there is considerable lack of coordination between sectors. Furthermore, at the district-level nutrition is often not a high priority and is insufficiently integrated into activities. The health sector primarily focuses on improving infant and young-child feeding while the agriculture sector focuses on food production, processing, and storage. There is considerable need to educate district-level actors involved in agriculture on the important role this sector can play in improving nutrition beyond reducing poverty and improving livelihoods.
- Low dietary diversity and intake of animal-source foods are key issues that require addressing availability, access, and consumption. Vegetable gardens are common and there are multiple crops and wild sources of nutrient-rich foods, but yields are low, inconsistent, and reliant on seasonal rainfall. Most rural populations are not aware of the nutritional content of the foods that they produce, gather, and subsequently consume and/or sell. While fish is a regular part of the Sierra Leonean diet, it is consumed in small quantities and is subject to seasonal variation. It is therefore not contributing adequate protein and micronutrients to diets. Most other animal-source foods are limited to special occasions and/or are sold as a key source of income.
- Poor water, sanitation, and hygiene practices make transmission of fecal-oral pathogens a widespread issue. Awareness and infrastructure for water, sanitation, and hygiene exist, but consistent and widespread use of key WASH practices is lacking. Animals generally roam freely in the yard and inside the house and children often play in the same areas as livestock, presenting an increased risk of fecal oral contamination. Additionally, food safety is a serious concern with unsanitary conditions at markets (fly infestation, spoiled fish and meat).
- Gender roles are also of concern. Women’s workload is significant, compromising feeding and care practices. Women’s role in decision-making is limited. Husbands and other family members are large influencers of IYCF practices and determine families’ access to health services.
- Availability and access to inputs are major constraints to farmers increasing productivity and improving food security. The MAFFS currently heavily intervenes in the fertilizer and seeds sub-sectors. The persistent distribution of large quantities of free and subsidized inputs by NGOs and government distorts markets and makes them non-competitive for the private sector.
- The current capacity of ABCs, FBOs, and village savings and loan associations (VSLAs) is weak and insufficient to achieve desired crop yields and increase crop diversity. Technical and business practices require improvement and there is a need for better market linkages. The Agriculture Extension Division is understaffed and the current staff lack transportation to the field and do not have access to adequate training or materials to do the work. Knowledge of agriculture practices and nutrition among trainers and recipients is lacking and there is a need to improve curricula and training. In addition, the content and quality of MSGs activities need to be improved and more strategic linkages to other community-based groups (ABCs, FBOs, and VSLAs) are needed to maximize women’s empowerment and nutritional outcomes.
- Relationships between the network of health services and hard-to-reach communities is a challenge for multiple reasons, including transport costs, some residual mistrust related to EVD, issues relating to fees for services, and health staff workload. The health system, especially at the health-clinic and health-post levels closest to rural populations, is weak in areas of communication, supervision, procurement, and reporting functions.
- One of the primary channels of mass communication is radio. These radio devices are generally under the control of men. Women rarely have access to radios. Access to newspapers and televisions by both women and men is limited. Mobile devices also are not common among the poorer communities. In addition, the literacy rates of rural men and women are very low, thus requiring careful consideration when developing Information Education Communication (IEC) materials.
Summary of Key Opportunities
Several medium- and long-term opportunities exist to improve the nutrition situation in Sierra Leone using an approach closely aligned with current national and district efforts. These opportunities would allow for initial ‘entry points’ for interventions and program activities to ensure a greater chance of integration and successful adoption with targeted program beneficiaries. These opportunities can be harnessed by multiple partners working together to leverage targeted resources:
- Stakeholders recognize the importance of nutrition and the multitude of nutritional challenges: Sierra Leone has demonstrated a growing commitment to improving nutrition using a multi-sectoral approach by joining the SUN Movement in 2011 and developing a Food Security and Nutrition Policy and Implementation plan. This plan includes a number of nutrition-specific and nutrition-sensitive actions, which if fully implemented, would go a long way to improving nutrition. Moreover, key stakeholders generally understand the need to target not only socially and economically vulnerable populations, but also to focus on periods of vulnerability during the life cycle (including the first 1,000 days). Better coordination between sectors at the national and district levels can leverage resources and build capacity among front-line workers. Given the growing recognition of the important role of nutrition-sensitive agriculture on health status, there is a distinct opportunity to work with existing agriculture projects and service providers to make their activities more nutrition sensitive and encourage SBCC leading to improved nutrition outcomes. At the same time it is important to recognize that investment in nutrition-sensitive agriculture interventions alone will not decrease high-levels of stunting and anemia.
- Consumption of nutrient-rich fruits and vegetables as well as animal-source foods: Households typically have homestead gardens but the amount of nutrient-rich foods grown and consumed is limited. There is great interest from community members, extension staff, and associations to review opportunities to better manage the production and utilization of different locally grown crops throughout the year, which could lead to increased food diversity. Fish is a well-accepted nutritious food in the district and thus can potentially provide individuals with fatty acids and more bioavailable micronutrients. Since fish is readily available (with seasonal variation), households could be encouraged to consume more of it.
- Inland Valley Swamps (IVS) are under development: MAFFS, with support from partners, has embarked on a program to rehabilitate old irrigation schemes and develop selected new IVS. Developing IVS can increase year-round production of a wide variety of crops and increase crop yield. They could also include integrated fish production systems. Under the farming system of integrating crops, fish, and small ruminants, crops will benefit from the animal manure and fish droppings and conversely animals can consume some of the crop byproducts, including vegetables. The fish can also eat some of the weeds in the flooded paddies. The enhanced productivity has the potential to improve food security (affordability and diversity of nutrient rich foods) and increase farmers’ income.
- Community structures are in place: While the number of implementing partners in Tonkolili is limited, well-established community groups exist and extend into the most isolated areas of the district. There is a nucleus of FBOs, ABCs, other private sector groups, and inputs dealers/service providers in the target district that could be used as platforms to deliver nutrition messages (nutritional value of foods, appropriate storage and preservation for nutrient retention, and diversification of produce and diets) and nutrition-sensitive activities (growing a wider crop variety, cooking demonstrations, clinic gardens, and community gardens). Furthermore, the rapid scale-up of MSGs being supported by UNICEF and the MOHS could provide an excellent mechanism to deliver nutrition-specific and nutrition-sensitive agriculture interventions during the first 1,000 days (appropriate IYCF and health practices, community gardens, and cooking demonstrations).
- Market structures exist: While some markets are still closed or are experiencing slow participation as a result of EVD, successfully increasing farm productivity and dietary diversification – as recommended in this report – can be achieved by providing excellent market information and management. Social and behavior change communication efforts can be employed to not only improve the public’s demand for radio broadcasts regarding where and when to market their produce (to complement existing market information systems), but also for improved vendor, produce, and general market hygiene. The existing market structure provides an excellent forum for a communication campaign centered on nutritious local foods that can link producers, vendors, and consumers. A campaign of this nature can stimulate demand for locally available nutritious foods and contribute to efforts to enhance smallholder farmer contributions and private sector linkages.
- Ebola virus disease has resulted in strong coordinated SBCC efforts: Multi-channel messaging regarding EVD has increased awareness of hygiene and sanitation issues at the community level. This is the result of a strong and unified response from the government, donors, and implementing partners’ to invest in SBCC. Stakeholders have come together to establish distinct roles while harmonizing and disseminating EVD health messages (avoidance of consuming bush meat, handwashing, reporting illness to health staff) through targeted channels. This has led to consistent messaging, which has reached diverse audiences through a variety of forms, each reinforcing the other, and extending to remote and underserved areas. Lessons learned regarding technical content, production capacities, roles of community actors, and coordination are beginning to be carried over to other sectors to improve communication clarity and coverage. For example, the SUN movement has instituted a communications group, which is currently working to harmonize nutrition-related messaging. Building on this momentum, additional nutrition-specific and -sensitive actions can be promoted. Given the heavy influence of husbands and mothers-in-law in household decision-making, these groups should be the target audiences. Adolescent girls also represent an important primary audience for SBCC interventions, as they are often stigmatized and may not be fully integrated into existing MSGs and other community groups.
- Innovative community-based tools can be applied: Several recent and current efforts by the GoSL and partners are promoting improved nutrition-specific and -sensitive agriculture practices. These include training modules developed by SLARI; nutrition training for health, agriculture, and veterinary extension agents; efforts to define dietary guidelines; SNAP materials; and the adaptation of LANNs training modules. The cumulative benefits of these materials can be harnessed to design training modules which engage and motivate community members, extension agents, health facility staff, and decision makers. Despite limited access to radio and TV in the district, there are a number of innovative community-based tools currently being tested and promoted globally that can be used to improve nutrition-specific and –sensitive messaging in rural areas. There is an opportunity to engage with existing social structures in Tonkolili using new and innovative tools for nutrition SBCC (i.e., literacy/numeracy training, radio or recorded listening sessions, video production and dissemination opportunities, and/or theater tours).
Programmatic Recommendations
Based on the findings in previous sections, SPRING proposes the following recommendations for USAID as potential entry points to affect nutrition within its medium- to long-term Feed the Future strategy. In addition to suggested beneficiaries, geographic zones of influence, partnerships to be developed, and technical intervention areas and illustrative activities, SPRING proposes a set of Feed the Future input, outcome, and impact indicators (Annex 3) that will allow USAID to track programmatic performance results for nutrition and nutrition-sensitive agriculture.
Target Beneficiaries
During the nutrition assessment, SPRING identified several key types of beneficiaries for targeted investments and interventions under Feed the Future for nutrition and nutrition-sensitive agriculture programming:
- Vulnerable community members, with particular emphasis on the first 1,000 days and 1,000-day households:
- adolescent girls
- young women of reproductive age (WRA)
- pregnant and breastfeeding mothers
- children, 0-59 months
- husbands, mothers-in-law, and mothers as primary caregivers of children
- Community groups:
- producer groups: FBOs, ABCs and other producer/market cooperatives, and VSLAs
- women’s groups: Mother Support Groups (MSGs) and Linking Agriculture, Nutrition and Natural Resources (LANN) Groups
- Youth Groups
- Health service providers:
- health care workers at health centers and posts at Chiefdom/District level,
- community Health (outreach) Workers
- traditional Birth Attendants
- Agriculture service providers:
- agricultural extension as well as community development agents at Chiefdom/District level;
- private sector suppliers and buyers
Proposed Zone of Influence (ZOI)
USAID/Sierra Leone was clear in its stated interest to target investments in Tonkolili District. For this reason, SPRING focused most of its fieldwork in Tonkolili, but also built an understanding of programming priorities and activities in the Northern Region through meetings with key NGO and government offices in Bombali. With markets in Bombali being the first point of entry for a range of horticultural commodities entering Sierra Leone from Guinea (LEO Project 2015), the linkage between Bombali’s primary market in Makeni and improved nutrition outcomes in Tonkolili are obvious; strengthened outcomes for agricultural income AND improved supply of more nutrient-rich foods for Tonkolili will rely, in part, on market activities in both districts.
Potential Partners and Networks
SPRING found several actors currently working on agriculture and nutrition programs that can contribute to continuing, expanding, and strengthening their support to vulnerable communities. A summary of the range of stakeholders undertaking nutrition-related programming in Tonkolili and Bombali is provided in Annex 4. In considering future investments in nutrition, potential partnerships include—
- implementing NGOs, such as Caritas, Concern, ACTS
- FBOs ABCs, MSGs, and VSLAs (for service delivery)
- learning institutions—
- Sierra Leone Agricultural Research Institute
- Njari University
- national/district level fora—
- national WASH consortium
- district WASH collaboration
- district SUN network
- national Federation of Farmers in Sierra Leone
- Sierra Leone Chamber for Agribusiness Development.
Suggested Strategies and Interventions
In developing the following recommendations for action, SPRING drew from its work in applying the conceptual pathways between agriculture and nutrition (figure 9). These pathways help to describe the range of opportunities that exist for agriculture to more effectively contribute to nutrition outcomes. They also remind us, however, that agriculture cannot, on its own, ensure sustained reductions in undernutrition. Strategic and purposeful linkages to nutrition-specific or direct determinants of nutrition, including health status and nutrient intake are critical to prioritizing nutrition-sensitive agriculture strategies and interventions. Key leverage points for nutrition require an enabling environment conducive to knowledge and learning as well as drivers of sustainability such as through local capacity building, protection of natural resources (water, soils, forests), and strengthening of the food market environment. While agriculture may be seen only as a source of diverse nutritious foods and income, in reality its effect on nutrition is multifaceted.
Firstly, agriculture supports a healthy, active life by producing (quantity and quality) foods within and for household consumption and for supplying foods to local markets. Secondly, agriculture as a livelihood source provides income (with a focus on quantity, timing and duration) to purchase food and health care. Thirdly—and an equally important though less obvious pathway from agriculture to nutrition—is the way agricultural livelihoods affect gender relations and the status of women. Women’s time availability, energy expenditure, and access to and control over productive resources and household income affect their own and their children’s health and nutrition status.
Figure 9. Conceptual Pathways between Agriculture and Nutrition
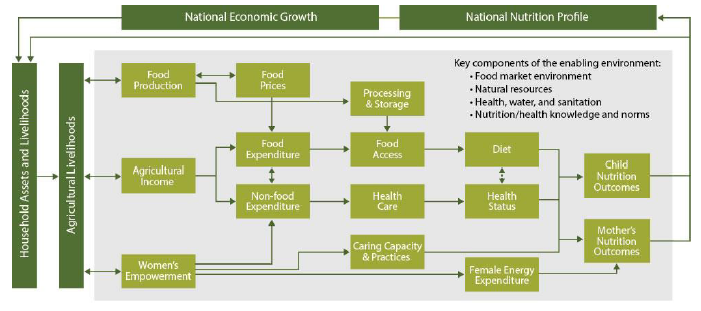
These key pathways regularly interact and are not always linear. The figure presented above shows how various agricultural investments or activities could improve access to food and health care, how they affect and are affected by the enabling environment, and how they ultimately affect the nutrition of women and children, who are considered the most vulnerable groups.
The following recommendations strive to address opportunities for improving nutrition along each of the pathways as well as for strengthening the enabling environment for nutrition through agriculture and the health and WASH sectors. Together, they comprise a multi-sectoral strategy for USAID’s investments in Sierra Leone.
Key Recommendations
SPRING proposes the following recommendations for USAID as potential entry points for the development of a medium- and long-term Feed the Future strategy.
- Continue to promote a multi-sectoral approach to nutrition across and among government institutions and other stakeholders by building capacity and strengthening coordination among key actors at the national and district-level.
- Target beneficiaries/clients: MOHS, MAAF, and other implementing partners
- Support in-depth analyses to further understand the immediate (e.g., investigating whether iron deficiency is a problem in Sierra Leone), basic, and underlying causes of malnutrition.
- Conduct a formal assessment of the progress of the National Food and Nutrition Security Implementation Plan 2012-2016 and use new data that includes nutrition-sensitive indicators monitored across sectors to develop the next iteration of the plan.
- Support the MOHS to establish a National Anemia Working Group under the SUN Movement.
- Undertake widespread capacity building to create personnel adequately trained in food and nutrition.
- Provide training to district-level actors involved in agriculture and health on the important role each sector can play in improving nutrition, especially in light of the competing demands and limited incentive for collaboration.
- Increase active participation in national and district-level SUN network and coordination bodies, promoting an appreciation for an integrated perspective of food security, nutrition, and agriculture.
- Secondment of nutrition technical resources to MOHS and MAFF to better link nutrition and agriculture activities by supporting policy revisions, integrating communications and M&E plans, and training implementing actors.
- Coordinate and prioritize which community groups (LANNs WGs, FBOs, MSGs, and VLSAs) should be receiving which types of nutrition-specific and -sensitive messages and activities, and establishing appropriate synergies to include shared training of field agents.
- Nutrition-specific and nutrition-sensitive interventions accomplish synergistic goals and must be implemented in the same geographic area in order to achieve optimal nutrition outcomes.
- Build on other program successes, test community-based models that integrate nutrition, gender, agriculture, and sanitation in select chiefdoms.
- Target beneficiaries/clients: MOHS, MAAF, and other implementing partners
- Support productivity improvements in community and household food production systems, emphasizing the production and consumption of diverse nutrient-rich foods, including vegetables and animal source foods.
- Target beneficiaries/clients: MSGs, FBOs
- Increase supply of and access to more nutritious/diverse foods
- Food production—
- Support the development and dissemination of improved breeds of livestock (especially small ruminants) and the development and/or evaluation of certain local germplasm and foreign materials/crops by the Sierra Leone Agricultural Research Institute (SLARI) and its collaborating institution, Njala University.
- Promote diverse crop and livestock integration especially of vegetables, fish, poultry and small ruminants to complement staple food (rice, cassava, etc) production, while mitigating risks, as a food security and resiliency strategy.
- Support development of community and backyard fishponds and vegetable gardens and improved poultry raising.
- Link to SBCC efforts to increase consumption of nutrient rich foods.
- Link to efforts to improve availability and access to inputs (seeds and fertilizers).
- Promote the safe processing, preservation, storage and preparation of nutrient-rich foods, particularly vegetables and animal source foods, for year-round availability and access at the household and community levels.
- Promote small-scale fish production, safe processing and preparation to maximize nutrient retention suitable for complementary feeding and year-round household consumption.
- Promote key biofortified crops such as cassava and orange-fleshed sweet potatoes noting that these varieties will require significant SBCC to change preferences to a food that is a different color, texture, and requires changes in cooking times. Increase the availability of diverse technologies including nutrient-rich crops in partnership with SLARI.
- Support MAFFS and other partners’ efforts for the rehabilitation of existing irrigation schemes and the development of new inland valley swamps to support year-round diverse food production and availability.
- Income generation (year-round)—
- In trainings, include income diversification, savings and household allocation strategies that favor purchase of nutritious foods, and other health seeking behaviors such as investment in care resources, and access to health services and a hygienic environment.
- Support and advocate for greater private sector businesses and associations’ participation in input supply, extension and advisory services rather than direct MAFFS provision/subsidizing.
- Encourage members of farmer organizations to use weekly markets (lumas) as aggregation points for crop sales, including more nutrient-rich horticultural and fruit crops.
- Support the necessary capacity enhancement of organizations in the business of horticultural crops (especially among women and youth) to lower costs of production and maximize earnings through bulk purchase of inputs, identification of key buyer quality, timing and quantity demands, and use of improved storage/preservation and packaging (value-addition) practices.
- Provide training and material support for entrepreneurial activities for men and women, which address nutrition, health, agriculture, and marketing (for example, soap manufacture, market transportation, food processing).
- Food production—
- Increase demand for more nutritious foods/diets
- Social and behavior change communication on consumption of vegetables and animal source proteins, sourced through home production and/or market purchase.
- Link to vegetable production and diverse farming systems efforts, including ensuring availability of inputs.
- Undertake formative research to better understand barriers and mitigations to overcome food taboos, especially those related to nutritious foods that should be consumed by pregnant and lactating women and children under-two years of age.
- SBCC to improve awareness of food safety threats and opportunities at all levels of the value chain including production, storage, transport, preparation and consumption.
- Promote and disseminate the newly developed Sierra Leone dietary guidelines.
- Design a communication strategy using information collected from formative research to promote nutrition specific behaviors and nutrition sensitive agriculture practices among priority beneficiary groups. Include in this strategy testing for new technologies, including the use of community video and pico projectors.
- Women’s empowerment—
- Explore options/experience with labor-sharing schemes to support more equitable distribution of labor, stressing the time allocation and energy expenditure of women, particularly of pregnant and lactating women.
- Promote women’s labor- and time-saving agricultural practices and technologies and link these to practices for improving household care and feeding.
- Ensure equitable access to irrigated or more productive lowlands for women to increase and improve horticulture crop production (a sub-sector dominated by women).
- Design and pilot nutrition-specific and nutrition-sensitive fora for husbands and mothers-in-law, and monitor impact for scaling-up and/or inclusion in national policies and/or FBO training.
- Link agriculture and nutrition activities to activities that reduce early marriage and pregnancy, such as girls’ access to education, women’s literacy programs, and increase women’s livelihoods and decision-making power.
- Facilitate capacity building of various private agricultural sector stakeholders, and align them with food and nutrition security priorities.
- Target beneficiaries/clients: FBOs, ABCs, private enterprises such as input wholesalers and agro-dealers, and agricultural associations such as the National Federation of Farmers in Sierra Leone, and the Sierra Leone Chamber for Agribusiness Development (SLeCAD)
- Conduct capacity and needs assessment of private agricultural stakeholders related to nutrition-sensitive agriculture such as nutrient-rich food supplies/inputs, safety and health standards, accessibility to women, and training capacity of dealers regarding nutrition-sensitive agriculture practices.
- Upgrade technical, business management, and profitability skills of target agricultural stakeholders to support nutrition. This could include preparing simple business plans and proposals, agricultural finance, product packaging, nutrition labeling, customer relations, advocacy, and produce processing to reduce women’s workload.
- Promote dietary diversity, food safety, sustainable agricultural production and processing practices, and other relevant nutrition-sensitive messages across all agricultural extension and advisory services, including those by FBOs, MSGs, and VSLAs and among farmer field schools, harmonizing messages, as appropriate with key nutrition-specific materials.
- Promote the production and consumption of diverse, nutrient-rich foods through market systems, such as—
- post-harvest processing to enhance nutrient retention
- fortification (e.g., rice)
- expanding markets for nutrient-rich foods (e.g. nutrient-rich foods such as vegetables and animal source protein foods, soy blended foods, fortified varieties of cassava, orange-fleshed sweet potatoes)
- strengthening connections to nutrition with any planned horticulture value chain strengthening activities per the Leveraging Economic Opportunities (LEO) report (July 2015)
- apply behavioral economics (e.g. “Nudge”/SBCC) strategies to support these efforts.
- Support the development of a private input supply sector and discourage market-distorting direct interventions through free and subsidized input distribution directly to farmers.
- Link Feed the Future strategies in Sierra Leone to the USAID/West Africa Regional Mission’s West Africa Seed Alliance (WASA) to support development of a stronger (private) local seed production and input (fertilizer) supply sector (as in Mali and Ghana).
- Through WASA, produce a GIS map of all agro-dealers in Sierra Leone, including the products they market (e.g., seed and veterinary drugs), to help farmers locate the products they need from the closest possible agro-dealer.
- Obtain support from the Regional Mission under its regional fertilizer program.
- Promote food safety and hygiene along food value chains, particularly among market retailers and food vendors.
- Target beneficiaries/clients: FBOs, ABCs, private enterprises such as input wholesalers and agro-dealers, and agricultural associations such as the National Federation of Farmers in Sierra Leone, and the Sierra Leone Chamber for Agribusiness Development (SLeCAD)
- Support direct implementation of nutrition and infection-mitigation interventions with a focus on promoting WASH and establishing a functional health system to ensure improved nutrition outcomes:
- Target beneficiaries/clients: Health clinic staff, CHWs, TBAs, MSGs
- Increase ANC attendance and services by encouraging women to attend throughout their pregnancy and not just at delivery (via CHWs, TBAs, community leaders, Lead Mothers, MSGs).
- Ensure essential drugs are available (iron-folic acid supplementation, deworming pills, and malaria drugs).
- Increase coverage of children’s six-month contact-point, ensure children receive zinc supplements in the management of diarrhea, vitamin-A supplementation, increased vaccination coverage, and deworming medication.
- Expand mobile health outreach services in rural communities.
- Improve SBCC (especially counseling in clinics) on appropriate IYCF practices, family planning, and iron-folic acid supplementation and free vs. fee-for-services, including assessing how to better coordinate designated service days. For example, rather than exclusively providing family planning counseling, integrate this service with child growth monitoring services.
- Support procurement and roll-out of rapid test kits by CHWs for malaria, to address anemia.
- Support the GoSL’s establishment of MSGs
- Ensure adolescent mothers are included.
- Improve group management and develop nutrition-specific and sensitive topical content.
- Include husbands and mother-in-laws through their participation in expanded MSGs or by creating synergies with the FBOs.
- Support the maintenance of newly improved WASH behaviors and promote safe play areas (e.g., clean play spaces, tippy taps, homemade soap, and proper handling of food and child feces).
- Improve PHU reporting and monitoring capabilities so that the data is correct and more useful for analyses.
- Target beneficiaries/clients: Health clinic staff, CHWs, TBAs, MSGs
Footnotes
1 GoSL has not adopted the 2011 WHO recommendation not to provide vitamin A supplementation post-partum.
References
acaps. 2015a. “Ebola Needs Analysis Project: Sierra Leone Multi-Sector Needs Assessment Report.” http://www.acaps.org/img/documents/m-acaps-enap-multi-sector-needs-assessment-sierra-leone-april-2015.pdf.
———. 2015b. “Ebola Outbreak Monthly Overview.” http://acaps.org/img/documents/m-acaps-monthly-overview_ebola-west-africa_4-may-2015.pdf.
———. 2015c. “WASH in Guinea, Liberia, and Sierra Leone: The Impact of Ebola.” Thematic Note.
AED. 2009. “USAID Office of Food for Peace Sierra Leone Food Security Country Framework FY 2010 – FY 2014.” Washington, D.C.: Food and Nutrition Technical Assistance II Project (FANTA-2), Academy for Educational Development (AED).
CFSVA. 2011. “State of Food Security and Nutrition: Sierra Leone 2011.” Comprehensive Food Security and Vulnerability Analysis (CFSVA). World Food Programme, Republic of Sierra Leone, UNICEF, European Union. http://documents.wfp.org/stellent/groups/public/documents/ena/wfp250158.pdf.
CIA. Continually updated. “The World Factbook: Sierra Leone.” Central Intelligence Agency.
DHS. 2014. “Sierra Leone Demographic and Health Survey 2013.” Freetown, Sierra Leone and Rockville, Maryland, USA: SSL and ICF International: Statistics Sierra Leone (SSL) and ICF International.
EngenderHealth. 2011. “The SEED Assessment Guide for Family Planning Programming.” New York.
FAO/WFP. 2014. “Crop and Food Security Assessment - Sierra Leone.” Special Report I4279E. FAO, WFP.
FEWS NET. 2013. “Sierra Leone Seasonal Calendar: Typical Year.”
Fofanah, Abu Bakarr. 2015. “High Level Overview: Health Sector Ebola Recovery Plan.” presented at the “From EBOLA to More Resilient Health Systems,” April 17.
Fongar, Andrea. 2014. “LANN Sierra Leone in Tonkolili and Kenema District: Cross-Sectional Baseline Survey Final Draft Report.” Welthungerhilfe, Irish Aid, Concern Worldwide.
Freedom House. 2012. “Countries at the Crossroads 2012: Sierra Leone.”
Gillespie, Stuart, Lawrence Haddad, Venkatesh Mannar, Purnima Menon, and Nicholas Nisbett. 2013. “The Politics of Reducing Malnutrition: Building Commitment and Accelerating Progress.” The Lancet 382 (9891): 552–69. doi:10.1016/S0140-6736(13)60842-9.
GoSL. 2002. “National HIV/AIDS Policy for Sierra Leone.” Government of Sierra Leone.
———. 2009a. “National Sustainable Agriculture Development Plan 2010-2030: Sierra Leone’s Comprehensive African Agriculture Development Programme.” Republic of Sierra Leone.
———. 2009b. “Free Healthcare Services for Pregnant and Lactating Women and Young Children in Sierra Leone.” Freetown, Sierra Leone: Government of Sierra Leone.
———. 2012a. “National Health Sector Strategic Plan 2010 - 2015: Joint Programme of Work and Funding (JPWF) 2012-2014.” Government of Sierra Leone Ministry of Health and Sanitation.
———. 2012b. “Food and Nutrition Security Policy Implementation Plan 2012-2016.” Government of Sierra Leone.
———. 2013. “The Agenda for Prosperity: Sierra Leone‘s Third Generation Poverty Reduction Strategy Paper (2013 – 2018).” Government of Sierra Leone.
———. 2015. “National Ebola Recovery Strategy for Sierra Leone: 2015-2017.” Government of Sierra Leone.
LEO Project. 2015. “Sierra Leone Agricultural Value Chain Analysis - Draft V.2: Animal Protein, Grains, Horticulture, and Legumes/Pulses in the Bombali and Tonkolili Districts.” USAID Leveraging Economic Opportunities (LEO) Project.
Mayhew, Melanie. 2015. “On Ebola Response and Recovery, World Bank and Partners Keep Pressure On.” World Bank. http://www.worldbank.org/en/news/feature/2015/04/16/on-ebola-response-recovery-world-bank-and-partners-keep-pressure-on.
MOHS. 2011a. “Sierra Leone Malaria Control Strategic Plan 2011-2015: Access to Malaria Control for All.” Government of Sierra Leone Ministry of Health and Sanitation.
———. 2011b. “Sierra Leone: Reproductive, Newborn and Child Health Policy 2011.” Sierra Leone Government Ministry of Health and Sanitation.
———. 2011c. “Sierra Leone: Reproductive, Newborn and Child Health Strategy (2011 - 2015).” Sierra Leone Government Ministry of Health and Sanitation.
———. 2012. “Sierra Leone Food and Nutrition Security Policy 2012-2016.” Government of Sierra Leone Ministry of Health and Sanitation. https://extranet.who.int/nutrition/gina/sites/default/files/SLE%202012%20Sierra%20Leone%20Nutrition%20Policy%20pdf%20version.pdf.
NERC. 2015. “Ebola Outbreak Updates: October 14, 2015.” Freetown, Sierra Leone: National Ebola Response Centre (NERC), Government of Sierra Leone.
ODI. 2014. “Understanding Malnutrition and Health Choices at the Community Level in Sierra Leone.” 4. Researching Livelihoods and Services Affected by Conflict. Secure Livelihoods Research Consortium, Overseas Development Institute (ODI).
openDemocracy. 2015. “Bound to Violence: Young Lives in Freetown.” Accessed October 15. http://www.opendemocracy.net/elisa-dari/bound-to-violence-young-lives-in-freetown.
Perez-Escamilla, R., L. Curry, D. Minhas, L. Taylor, and E. Bradley. 2012. “Scaling Up of Breastfeeding Promotion Programs in Low- and Middle-Income Countries: The ‘Breastfeeding Gear’ Model.” Advances in Nutrition: An International Review Journal 3 (6): 790–800. doi:10.3945/an.112.002873.
Peter Davis. 2015. “Ebola in Sierra Leone: Economic Impact & Recovery.” Sierra Leone Opportunities for Business Action (SOBA), DFID, Adam Smith International. http://www.adamsmithinternational.com/documents/resource-uploads/Ebola_in_Sierra_Leone.pdf.
Poraj-Wilczynski, Huw. 2015. “Needs Must as Sierra Leone Gets back to Business after Protracted Ebola Crisis.” The Guardian, May 8, sec. Global development. http://www.theguardian.com/global-development/2015/may/08/sierra-leone-ebola-crisis-economy-business-farmers.
Risso-Gill, Isabelle, and Leah Finnegan. 2015. “Children’s Ebola Recovery Assessment: Sierra Leone.” Save the Children, World Vision International and Plan International and UNICEF.
SLMN. 2013. “Sierra Leone Micronutrient Survey.” Freetown, Sierra Leone: MOHS, UNICEF, HKI, and WHO.
SMART Survey. 2010. “Report on The Nutritional Situation of Sierra Leone Nutrition Survey Using SMART Methods.” UNICEF.
———. 2014. “Sierra Leone National Nutrition Survey 2014.” Freetown, Sierra Leone: MOHS and UNICEF Sierra Leone.
SPRING. 2014. “A Landscape Analysis of Anemia and Anemia Programming in Sierra Leone.” Arlington, VA: USAID/Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) Project.
SUN. 2015. “Sierra Leone.” Scaling Up Nutrition (SUN). Accessed October 10. http://scalingupnutrition.org/sun-countries/sierra-leone.
UNDP. 2015a. “Sustaining Human Progress: Reducing Vulnerabilities and Building Resilience.” Human Development Report 2014: Summary. New York, NY: United Nations Development Programme. Accessed October 7.
———. 2015b. “UNDP in Sierra Leone.” United Nations Development Programme. Accessed October 7. http://www.undp.org/content/sierraleone/en/home/countryinfo.html.
UNICEF. 2013. “Annual Report 2013: Sierra Leone.” UNICEF. http://www.unicef.org/about/annualreport/files/Sierra_Leone_COAR_2013.pdf.
———. 2015. “Sierra Leone Health Facility Survey 2014: Assessing the Impact of the EVD Outbreak on Health Systems in Sierra Leone (draft).” Accessed September 28. http://www.unicef.org/emergencies/ebola/files/SL_Health_Facility_Survey_2014Dec3.pdf.
WB. 2015a. “Sierra Leone: Data.” World Bank. http://data.worldbank.org/country/sierra-leone.
———. 2015b. “Sierra Leone Overview.” The World Bank. October 5. http://www.worldbank.org/en/country/sierraleone/overview#1.
WFP. 2015a. “Emergency Food Security Assessment: Sierra Leone.” World Food Programme. http://documents.wfp.org/stellent/groups/public/documents/ena/wfp276779.pdf.
———. 2015b. “Food Insecurity on the Rise as Ebola Abates: Application of Shock Impact Simulation Model (SISMod) to Measure Ebola’s Economic Impacts on Hunger.” World Food Programme. http://documents.wfp.org/stellent/groups/public/documents/ena/wfp275534.pdf.
WHH, FAO, MAFFS. 2014. “Ebola in Sierra Leone: The Impacts of the ‘Ebola Virus Disease’ on the Livelihoods of Rural Communities, Agricultural Production and Food Security.” Deutsche Welthungerhilfe e.V., Ministry of Agriculture Forestry and Food Security (MAFFS), FAO Sierra Leone.
Appendices
Please download the report using the link at the top of the page to view appendices.