
Nigeria ranks 152 of 188 countries in the 2015 Human Development Index and is identified as the country with the third-highest absolute number of children who are stunted in the world. According to the 2013 Nigeria Demographic and Health Survey, 37 percent of Nigerian children under five years of age are stunted (NPC and ICF International 2014). USAID | Nigeria’s buy-in to SPRING through the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) presented an opportunity to reverse these trends, given that malnutrition is worsened in the context HIV and AIDS.
We began work in Nigeria in June 2012 with the goal of reducing undernutrition, preventing stunting, and working with women and children to reduce anemia in Benue State and the Federal Capital Territory (FCT). In FY14, we revised our programmatic goal in response to USAID’s efforts to improve nutrition and food security outcomes within their PEPFAR-funded programs for orphans and vulnerable children (OVC) and we focused on reducing maternal and child undernutrition and improving HIV-free survival of infants and young children.
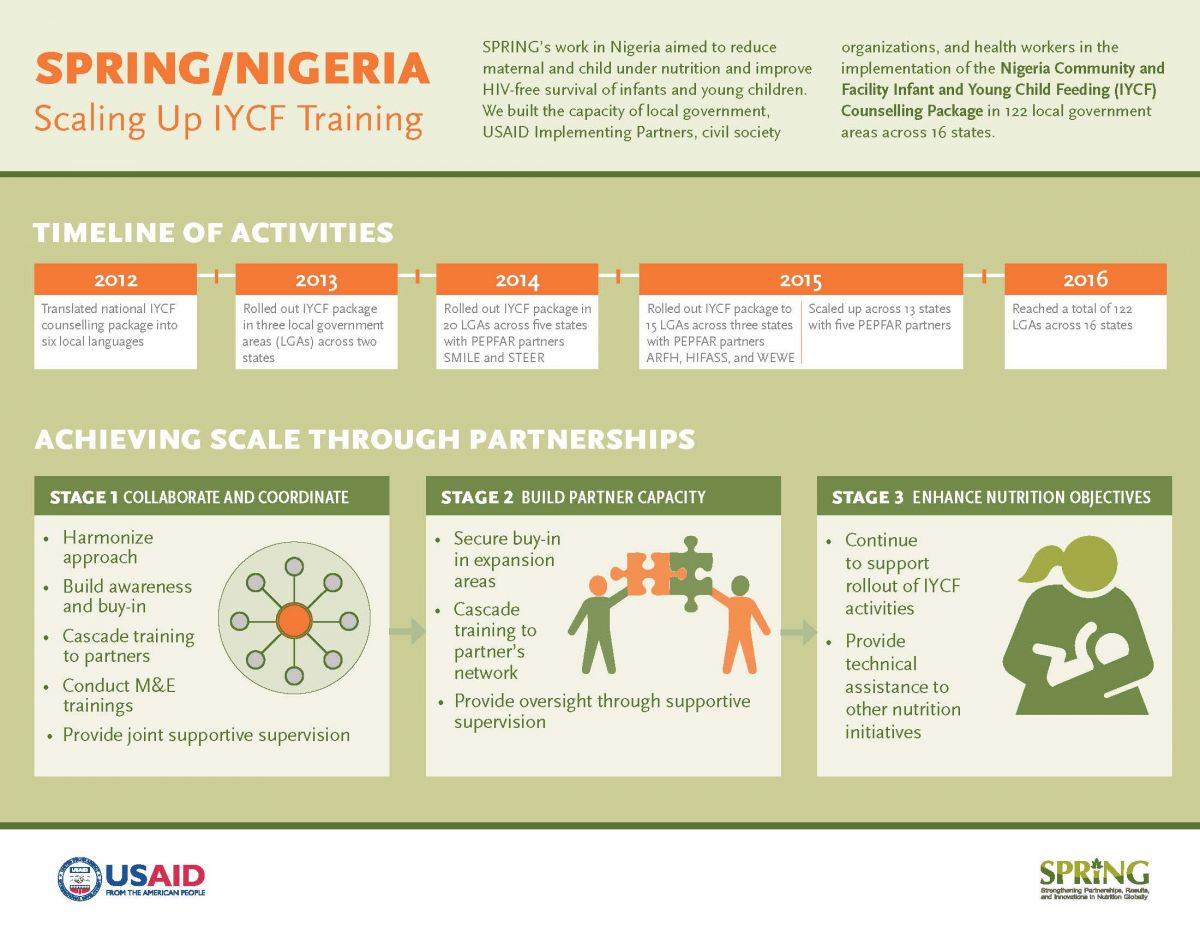
SPRING’s approach raised awareness and improved infant and young child feeding (IYCF) by building capacity in the use of the Infant and Young Child Feeding Counselling Package in facilities (F-IYCF) and the Community Infant and Young Child Feeding Counselling Package in communities (C-IYCF) throughout the country.
Building on USAID | Nigeria’s earlier investments in the Infant and Young Child Nutrition (IYCN) project, SPRING supported the development of tools and materials that strengthened the capacity for and delivery of IYCF. As a result, Nigeria has harmonized policies and training and counselling tools to support the integration of IYCF interventions into existing maternal and child care services, including the prevention of mother-to-child transmission (PMTCT) of HIV.
We helped five PEPFAR-funded OVC implementing partners meet and enhance their nutrition and food security-related objectives by rolling out the national IYCF counselling package in their implementation areas. Our strategy built the capacity of OVC partners, civil society organizations (CSO), and government counterparts on IYCF through sensitization and advocacy, training, supportive supervision, and by strengthening coordination and collaboration among these actors.
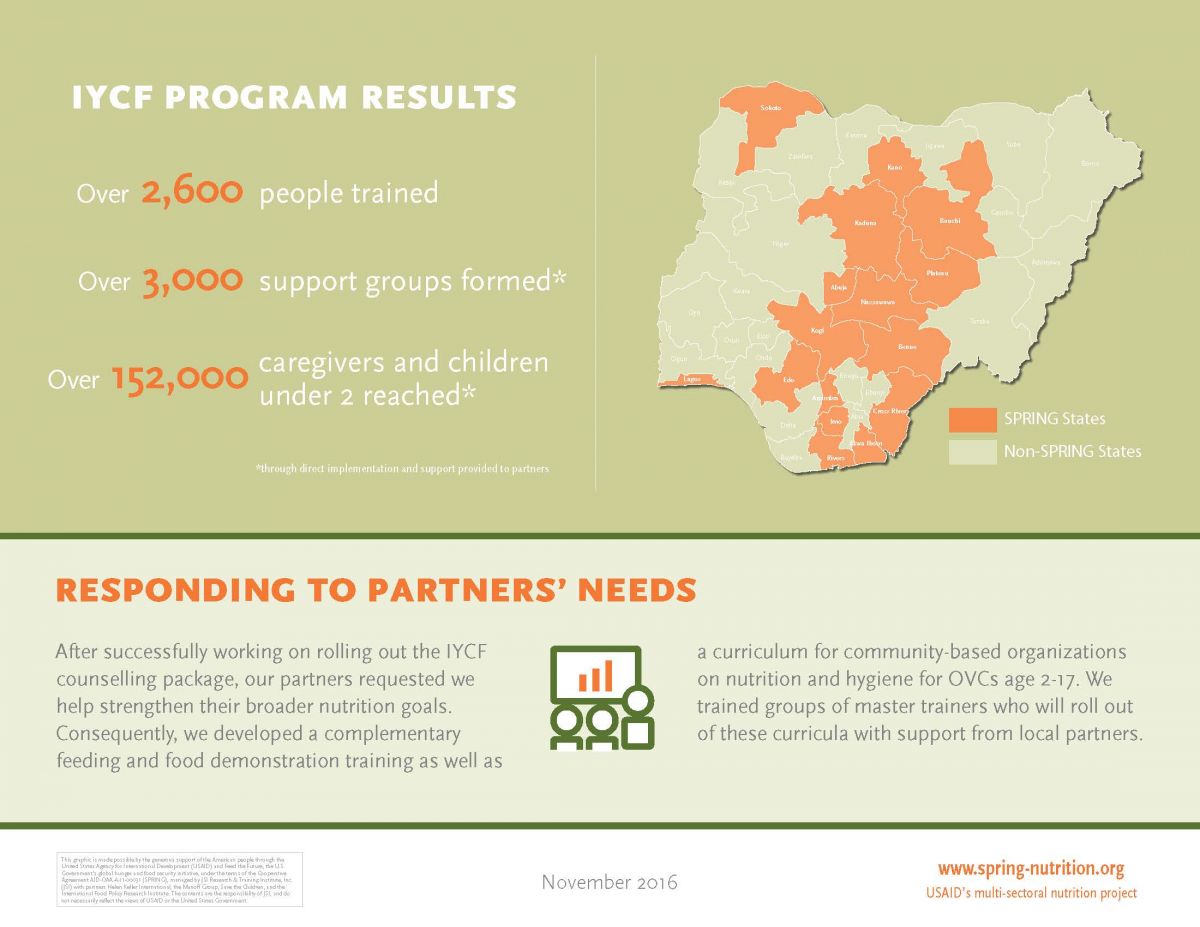
We provided technical assistance to the groups listed in box 1 and scaled up the IYCF counselling package (community and/or facility package) across 122 local government areas (LGAs) in 16 states spread across all six geopolitical zones (Akwa-Ibom, Anambra Bauchi, Benue, Cross River, Edo, Federal Capital Territory [FCT], Imo, Kaduna Kogi, Kano, Lagos, Nasarawa, Plateau, Rivers, and Sokoto). The partnerships have created strong links between the government and the OVC partners and their CSOs at the community level, thereby increasing ownership and support of IYCF activities within the states and LGAs. Our efforts established a foundation for building capacity and strengthening systems, which also has created community demand for IYCF services.
Box 1. Groups Receiving Technical Assistance from SPRING/Nigeria
Government of Nigeria
- Ministry of Health
- Ministry of Women Affairs & Social Development
- Ministry of Budget and Planning
- Nigeria Primary Health Care Development Agencies
USAID Partners under UGM
- Sustainable Mechanisms for Improving Livelihoods Household Empowerment (SMILE)
- Systems Transformed for Empowered Action and Enabling Responses for Vulnerable Children (STEER)
USAID Partners under LOPIN
- Association for Reproductive and Family Health (ARFH)
- Health Initiatives for Safety and Stability in Africa (HIFASS)
- Widows and Orphans Empowerment Organization (WEWE) under the Local Partners for Orphans and Vulnerable Children (LOPIN) initiatives.
Through our five OVC partners, we worked with more than 100 CSOs, facilitated the formation of 3,280 IYCF support groups, and reached 153,174 caregivers and children under two. We also provided Centers for Disease Control and Prevention (CDC) implementing partners with a master training on both the community and facility IYCF packages. In total, we trained 2,678 people on one or both IYCF counselling packages and two other curricula developed by SPRING: Nutrition and Hygiene for Orphans and Vulnerable Children in Nigeria: A Training Guide for Community-Based Organisations and Nigeria: Complementary Feeding and Food Demonstration Training Package.
We worked with the government to strengthen coordination of IYCF activities by building on established structures within the states to ensure government ownership of IYCF rollout. This also ensured that planning and implementation of IYCF activities within the states and LGAs occurred in collaboration with the relevant government agency. Planning for and training in IYCF strengthened the capacity of the state and LGA nutrition focal persons. Supportive supervision and mentoring activities have improved the coordination system using resources from government coffers.
The results of our capacity and beneficiary assessment demonstrated that working at scale does not compromise implementation quality. More than 70 percent of CSOs, health workers, and community volunteers who were trained by SPRING over the course of the project retained high levels of knowledge on IYCF. More than 80 percent had favorable attitudes toward issues such as male involvement in support groups and in the home, women’s and children’s nutrition when the mother is HIV-positive, and breastfeeding among working women. Most offered favorable opinions and comments about support from SPRING and partners. The capacity built by SPRING appears to have led to high-quality program implementation, which in turn resulted in positive IYCF practices among support group beneficiaries. Additional findings from the assessment revealed that 66 percent of mothers of children less than six months of age interviewed were practicing exclusive breastfeeding, while 67 percent of nursing mothers expressed confidence in their ability to breastfeed their child for at least two years.
SPRING also improved the policy environment for nutrition programming by helping to harmonize nutrition monitoring tools, develop the National Policy on Food and Nutrition and Plan of Action, and review the National Strategic Plan of Action for Nutrition (2014–2019).
This report captures SPRING/Nigeria’s key accomplishments over five years of implementation.
Background
Promotion of optimal infant and young child feeding (IYCF) practices is critical to the prevention of nutrition-related morbidity (such as stunting) and mortality (Bhutta et al. 2013). Nigeria has the third-highest absolute number of children who are stunted in the world. According to the 2013 Nigeria Demographic and Health Survey (DHS), 37 percent of Nigerian children under five years of age are stunted (NPC and ICF International 2014). Despite the fact that breastfeeding is nearly universal in Nigeria (97 percent of children are breastfed), early initiation of breastfeeding is only 38 percent; 17 percent of children under the age of six months are exclusively breastfed; and only 10 percent of children age 6–23 months are fed in compliance with the IYCF recommendations (consuming breastmilk or other milk products as well as having the minimum dietary diversity and minimum meal frequency).
The most serious indicators of poor nutritional status are found in the northern regions of Nigeria, where the prevalence of stunted children (children with a Height-for-Age Z-score of -2 standard deviations from the median) is 29 percent in the North Central Region; 42 percent in the North East Region; and 55 percent in the North West Region, compared to 20 percent stunting in the South West and South-South Regions and 16 percent in the South East Region (NPC and ICF International 2014).
USAID | Nigeria’s buy-in to the SPRING project through the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) presented an opportunity to curb these trends, given that malnutrition is worsened in the context HIV and AIDS. The HIV epidemic influences child survival both directly through mother-to-child transmission and indirectly by diverting resources and attention from children to the care and treatment of a sick parent. The epidemic continues to weigh heavily on maternal and child mortality in countries like Nigeria, which had the highest number of new HIV infections (60,000) among children in 2012. There are an estimated 17.5 million orphans and vulnerable children (OVC) in the country (FMOH 2013; FMOWASD 2008; UNAIDS 2013). Furthermore, 10.7 percent of the 69 million children in the country are vulnerable (UNICEF 2006), and 10 percent are orphaned. A key challenge in Nigeria is to assist families and communities to care for these children in areas where the number of children who have or are affected by HIV has increased (FMOWASD 2008).
SPRING Goals and Objectives
We began work in Nigeria in June 2012 with the goal of reducing undernutrition, preventing stunting, and working with women and children to reduce anemia in Benue state and the Federal Capital Territory (FCT). In FY14, we revised our programmatic goal in response to USAID’s efforts to improve nutrition and food security outcomes within their PEPFAR-funded OVC programs by focusing on reducing maternal and child undernutrition and improving HIVfree survival of infants and young children in Nigeria. Overall, our activities focused on achieving four broad objectives:
- Increase access to nutrition information and counselling services in OVC project communities.
- Improve national social and policy environment regarding priority nutrition practices and services.
- Enhance the evidence base with respect to the community-based infant and young child feeding (C-IYCF) counselling package (with funding from USAID/Washington).
- Improve nutrition programming efforts to prevent undernutrition in OVC project communities.
Technical Approach
Building on USAID | Nigeria’s earlier investments in the Infant and Young Child Nutrition (IYCN) project, SPRING supported the development of tools and materials that strengthened the capacity for and delivery of infant and young child feeding and nutrition programs. Nigeria currently has training and counselling tools to support the integration of IYCF interventions into existing maternal and child care services, including the prevention of mother-to-child transmission (PMTCT) of HIV.
The Integrated Infant and Young Child Feeding Counselling Package for use in secondary and tertiary facilities (F-IYCF counselling package) and the Community Infant and Young Child Feeding Counselling Package (C-IYCF counselling package) were adapted from the United Nations Children’s Fund (UNICEF) and World Health Organization’s (WHO) generic global documents and the WHO’s 2010 National Recommendations on IYCF in the Context of HIV, following a series of technical working group meetings comprising all relevant government agencies, parastatals, development partners, and NGOs. The Nutrition Division of the Federal Ministry of Health (FMOH) led the process with financial support from UNICEF, the (former) IYCN, SPRING, and Working to Improve Nutrition in Northern Nigeria (WINNN) projects.
SPRING translated the C-IYCF counselling package into five Nigerian languages—Hausa, Idoma, Igbo, Tiv, and Yoruba—at the request of the FMOH, USAID, and other partners. Each translation was field-tested and reviewed before finalization. The Government of Nigeria approved the final training package, with an official launch in August 2013 by the FMOH as part of activities to commemorate that year’s World Breastfeeding Week.
SPRING’s approach focused on building capacity in both the F-IYCF and C-IYCF counselling packages, and scaling up implementation throughout the country. Since FY14, we have provided helped PEPFAR-funded OVC implementing partners (referred to as OVC partners) enhance their nutrition-related objectives by rolling out the C-IYCF package in their communities. Our strategy focused on building the capacity of OVC partners, their civil society organizations (CSOs), and government counterparts on IYCF through sensitization and advocacy, training, supportive supervision, and strengthened coordination and collaborative efforts between these various actors.
Despite global interest and uptake of both IYCF counselling packages, little is known about its effect on IYCF behaviors in the countries where it has been adapted. After consultations with SPRING and UNICEF, the FMOH agreed to support an evaluation of the package and share the findings nationally and internationally to inform future investments in IYCF programming. The main purpose of the evaluation is to assess the effectiveness of the C-IYCF counselling package in improving IYCF behaviors in an environment supportive of its design, management, technical assistance, and monitoring when adapted to local context and implemented at scale. While the evaluation is not nationally representative, the findings should help national-level decisionmaking in Nigeria. The results will also make an important scientific contribution to the field of nutrition, in which there is relatively little evidence on the impact of a large-scale C-IYCF counselling package intervention.
Interventions and Coverage
SPRING provided technical assistance to the Government of Nigeria through the Ministries of Health, Women Affairs & Social Development, and Budget and National Planning, as well as Primary Health Care Development Agencies. We also helped USAID partners Sustainable Mechanisms for Improving Livelihoods and Household Empowerment (SMILE) and Systems Transformed for Empowered Action and Enabling Responses for Vulnerable Children (STEER) under the Umbrella Grant Mechanism (UGM). Additional support was provided to the Association for Reproductive and Family Health (ARFH), Health Initiatives for Safety and Stability in Africa (HIFASS), and Widows and Orphans Empowerment Organization (WEWE) under the Local Partners for Orphans and Vulnerable Children (LOPIN) initiatives, as we scaled up the IYCF counselling package (community and/or facility components) across 122 LGAs in 16 states. These states—Akwa-Ibom, Anambra Bauchi, Benue, Cross River, Edo, FCT, Imo, Kaduna, Kogi, Kano, Lagos, Nasarawa, Plateau, Rivers, and Sokoto—are spread across all six geopolitical zones.
Through our five OVC partners, we worked with more than 100 CSOs, facilitated the formation of 3,280 IYCF support groups, and reached 153,174 caregivers and children under two. We also provided a master training on both the community and facility IYCF counselling packages to Centers for Disease Control and Prevention (CDC) implementing partners. In total, we trained 2,678 people on IYCF.
Map 1. SPRING/Nigeria’s Implementation Areas, by State

SPRING’s Implementation Areas, by LGA
| State | No. of LGAs | LGAs |
|---|---|---|
| Anambra | 3 | Ayamelum, Anambra East, Akwa North |
| Akwa-Ibom | 5 | Uyo, Oron, Ikot Epkene, Okobo, Uruan |
| Bauchi | 8 | Alkaleri, Bauchi, Ganjuwa, Katagum, Misau, Ningi, Tafawa-Balewa, Toro |
| Benue | 12 | Ado, Buruku, Gwer East, Gboko, Katsina Ala, Kwande, Makurdi, Oju, Opuku, Otukpo, Ukum, Vandeikya |
| Cross River | 13 | Abi, Akamkpa,Akpabuyo, Biase, Calabar South, Obubra, Obudu, Boki, Calabar Municipal, Etung, Ikom, Obalinku,Bekwara |
| Edo | 9 | Akoko Edo, Egor, Esan North East, Esan South East, Etsako West, Ikpoba- Okha, Oredo, Orhionmwon, Owan East |
| FCT | 3 | Amac, Bwari, GwagwaLada |
| Imo | 4 | Ohaji Egbema, Owerri-West, Ngor-Okpala, Okigwe |
| Kano | 10 | Bichi, Dala, Dambatta, Fagge, Gwarzo, Kano Municipal, Kiru, Nassarawa, Rano, Wudil |
| Kaduna | 9 | Chikun, Ikara, Jaba, Jamaa, Kachia, Kaduna North, Kaduna South, Zangon-Kataf, Zaria |
| Kogi | 11 | Bassa, Yagba East, Ofu, Okehi, Kabba-Bunu, Igalamela/Odolu, Dekina, Ankpa, Okene, Lokoja, Olamaboro |
| Lagos | 7 | Ajeromi, Badagry, Kosofe, Ojo, Badagry, Surulere, Apapa, Agege |
| Nasarawa | 7 | Akwanga, Keana, Lafia, Nasarawa, Nassarawa-Eggon, Obi, Toto |
| Plateau | 9 | Barkin-Ladi, Jos North, Jos South, Kanam, Langtang South, Mangu, Riyom, Shendam, Wase |
| Rivers | 3 | Obio-akpor, Port-harcourt, Eleme |
| Sokoto | 9 | Binji, Goronyo, Illela, Sabon-Birni, Silame, Tambuwal, Tureta, Wammako, Yabo |
Major Accomplishments
SPRING’s major accomplishments in Nigeria fall into four categories:
- Increased access to nutrition information and counselling services in OVC project communities
- Improved national social and policy environment for priority nutrition practices and services
- Enhanced evidence base for the C-IYCF Counselling Package
- Improved nutrition programming efforts to prevent undernutrition in OVC project communities.
Increased Access to Nutrition Information and Counselling Services in OVC Project Communities
SPRING’s single-most significant accomplishment is the scale-up of the facility and community IYCF packages across 16 states and 122 LGAs, training a total of 2,678 people and directly reaching a total of 165,295 through direct implementation and work with partners. We also provided copies of both the F-IYCF and C-IYFC counselling packages to representatives of all 36 states in the federation.
The C-IYCF counselling package rollout is based on a four-tier training cascade, culminating in the formation of support groups at the community level. Communities, LGAs, and states were selected in conjunction with the Federal Ministry of Health and the USAID implementing partners. Participants in the C-IYCF counselling package trainings were selected from the following: state and LGA representatives from the Ministry of Health (MOH), Federal Ministry of Women’s Affairs and Social Development (FMOWASD), and Ministry of Agriculture (MOA); OVC partner program staff; and the officer in charge from primary health care centers (PHCs) and community volunteers.
C-IYCF Training Cascade
Tier 1: State-level master trainers
Tier 2: LGA-level trainers and coaches
Tier 3: PHC staff and community volunteers
Tier 4: Formation of IYCF support groups
The facility-based infant and young child feeding (F-IYCF) training is designed to ensure that nutrition services are linked to and complement HIV-treatment protocols and systems; that nutrition services are integrated into the facility-based HIV services; and that there is consistency of messaging and counselling at the referral-facility level. Participants in the F-IYCF trainings were drawn from secondary and tertiary facilities: nutrition focal persons; matrons-in-charge from the pediatric ward, the under-five immunization clinic, the maternity ward, and the antenatal care unit; and nurses and doctors from the HIV unit. SPRING implemented the F-IYCF counselling package through FY14, at which point USAID requested that we focus on rolling out the C-IYCF counselling package.
We created a job aid to help community volunteers conduct support groups after they receive their training (Conducting an Infant and Young Child Feeding Support Group Meeting in Nigeria). The job aid is also intended to ensure that facilitators follow a standard process for conducting a support group meeting. It is designed to complement the IYCF counselling cards and key message booklet used by support group facilitators.
Advocacy and Sensitization on Infant and Young Child Feeding

Over the life of the project, SPRING conducted 123 sensitization meetings across 122 LGAs and 16 states, meeting with stakeholders at each level to gain access to the LGAs and communities. These meetings allowed us to raise awareness of optimal IYCF practices, change perceptions, and influence key stakeholders to intensify IYCF efforts and nutrition programming. We advocated for an increased budget for community-based nutrition activities (including rolling out the C-IYCF counselling package); established and strengthened structures for collaboration on IYCF programming efforts (by sharing SPRING’s experience in rolling out the counselling package in other areas); and adapted relevant national policies and guidelines on IYCF.
Meeting attendees included state committees on food and nutrition; senior government officials of the Ministries of Health, Agriculture and Natural Resources Women’s Affairs and Social Development; and Budget and Planning; chairs of local government administrations; LGA supervisors for health; state nutrition officers; LGA nutrition focal persons; social mobilization officers; and heads of LGA agriculture departments.

After rolling out the IYCF counselling package in a given area, we raised awareness of optimal IYCF practices at national and state events, such as World Breastfeeding Week, conducted in partnership with our OVC partners and their respective CSOs.
Building Capacity through Training
In FY13, in conjunction with the Department for International Development-funded Working to Improve Nutrition in Northern Nigeria (WINNN) project, we trained 26 people on the IYCF counselling package. This created a pool of trainers who could be called upon to help launch training cascades throughout the country. With the MOH in LGAs in Benue state and two area councils in FCT, we rolled out the F-IYCF and C-IYCF counselling packages, including training cascades and supportive supervision.
Since FY14, we have provided technical support to PEPFAR-funded OVC implementing partners, beginning with UGM partners STEER and SMILE, as we rolled out the F-IYCF and C-IYCF counselling packages. SPRING conducted all four tiers of the training cascade, ensuring that support groups were formed in the communities across 20 LGAs in five states: Bauchi, Benue, Edo, FCT, and Kaduna.
In FY15, we expanded the C-IYCF counselling package as these partners moved into new communities: 21 new LGAs in existing UGM project states and 47 additional LGAs in five new project states (Kano, Kogi, Nasarawa, Plateau, and Sokoto). We conducted state-level trainings for each of the UGM partners to build their capacity to roll out the C-IYCF counselling package in new implementation areas. The UGM partners cascaded the training at the LGA and community levels and ensured formation of IYCF support groups in their respective focal states.
In FY15, we began work with three additional PEPFAR-funded implementing partners under the LOPIN initiative: ARFH, HIFASS, and WEWE. Following the model established with UGM partners STEER and SMILE, we focused our first year on building the capacity of the LOPIN partners to roll out the C-IYCF counselling package as they moved into 15 LGAs in Cross River, Imo, and Lagos states. We conducted the entire training cascade (state and LGA levels) and facilitated the establishment of support groups in each of the focal states.
In our final year (FY16), we transitioned to a reinforcement role with the LOPIN partners and continued to provide overarching support and technical assistance to the UGM partners. We expanded the rollout of the C-IYCF counselling package to nine new LGAs in three new LOPIN project states of Akwa-Ibom, Anambra, and Rivers, conducting state-level trainings. LOPIN partners then cascaded the trainings to the LGA and communities and established support groups.
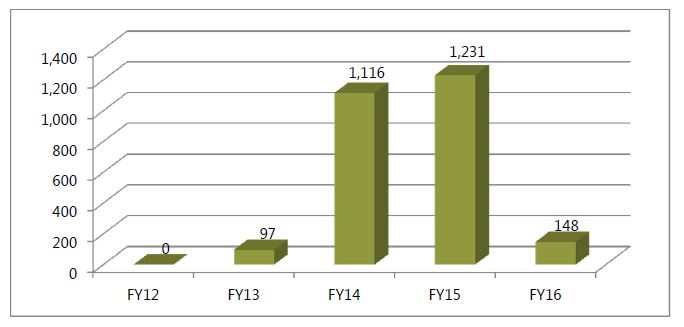
At the request of USAID, we trained 23 CDC implementing partner staff and their CSO partners as master trainers on the C-IYCF counselling package in FY16. We also trained 31 CDC implementing partner staff and their CSO partners as master trainers on the F-IYCF counselling package. The participants at these two trainings were from Benue, Nasarawa, and FCT states. Trained participants oversaw the rollout of the C-IYCF counselling package in the CDC priority LGAs in the aforementioned states. Participants trained in the F-IYCF counselling package are overseeing the integration of IYCF practices into HIV treatment protocols in their respective health facilities and ensuring the consistency of IYCF messaging and the quality of counselling services. The total number of participants trained by SPRING on IYCF (by fiscal year) is indicated in Figure 1.
Figure 1. Number Trained on IYCF by SPRING, by Fiscal Year
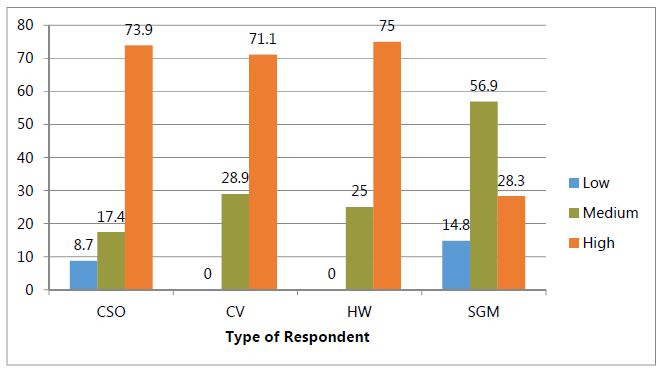
An aggregate analysis of the pre- and post-SPRING IYCF training assessment results show an average improvement in learning outcomes of almost 30 percentage points. Our 2016 assessment indicated that SPRING’s capacity-building approach has led to significantly improved knowledge and attitudes about counselling on optimal IYCF practices. Support group member (SGM) beneficiaries were also seen to have medium to high knowledge levels (see Figure 2).
Knowledge was assessed based on responses to 38 yes/no questions, with high being at least 70 percent correct, medium 50–69 percent correct, and low less than 50 percent correct. It is noteworthy that more than 70 percent of CSOs, health workers, and community volunteers had retained “high” knowledge levels at the time of the assessment, and almost all had at least medium levels of knowledge. The low levels of some CSOs were likely due to staff turnover, with new staff who had not yet been trained. To a large degree, knowledge was passed down to support group members, with over 85 percent demonstrating medium or high levels. Knowledge is a necessary but incomplete aspect of behavior change, so these results show encouraging potential toward that end. We also found that support group members, the ultimate beneficiaries of the C-IYCF counselling package trainings, reported practicing optimal IYCF behaviors at a higher rate than the 2013 Nigeria DHS. (See next section for more details.)
Figure 2. Assessed Level of C-IYCF Knowledge among Respondents, by Category of Respondent
Increasing Access to IYCF Services

As a result of the IYCF cascade trainings, community volunteers are able to establish support groups and provide caregivers with nutrition information and counselling on IYCF. We have established 3,280 IYCF support groups (295 through SPRING trainings and 2,985 through our support to OVC partners and their CSOs). Through our trainings, community events, supportive supervision, and support groups, we have reached 153,174 caregivers and children under two (41,105 through direct implementation and 112,069 via support to OVC partners).
Trained community volunteers, serving as IYCF support group facilitators, and CSO staff are the entry point to communities for IYCF information-sharing links to providing vital links with IYCF services at the PHC (where a staff member has also been trained). For example, SPRING-trained CSOs have integrated the identification and referral of cases of severe acute malnutrition into their community-based growth promotion and immunization programs. SPRING’s nutrition coordinators worked with LGA nutrition focal persons to establish referral and follow-up systems between facilities and community programs (such as IYCF support groups) and identified ways to improve the functioning of these systems.
Findings from our Assessment of SPRING-Supported IYCF Implementation in Nigeria—Measuring the Knowledge, Attitudes, and Practices of Partners and Care Givers, which assessed the capacities of trained partners and beneficiaries as well as the IYCF practices of target beneficiaries (support group members), showed that most beneficiaries had medium to high knowledge of IYCF concepts, positive attitudes, self-efficacy, and had begun to adopt positive practices. Table 2 shows women’s practices with their youngest child, followed by their reported confidence that they will use good IYCF practices in the future, including significant improvements in optimal feeding and care practices.
Table 2. IYCF Practices and Self-efficacy among Support Group Members—Percent Responding Positively to Each Question
| Indicators related to IYCF practices | Total % (N=371) |
|---|---|
| Self-efficacy: how confident was the woman that she would be able to… | Confident/very confident (%) N=297 |
| Fed youngest child colostrum | 91.1 |
| Began breastfeeding within 30 minutes after giving birth | 84.6 |
| Practicing EBF (only breastmilk in previous 24 hours) | 61.4 |
| Breastfeed a baby within 30 minutes of childbirth | 93.8 |
| Breastfeed exclusively for 6 months without any other food or drink | 96.3 |
| Introduce your baby to nutritious and safe and soft semi-solid foods at 6 months | 95.6 |
| Breastfeed your baby for at least 2 years | 67.3 |
| Mothers/caregivers should be alert or responsive to infants/child signs that s/he is ready to eat | 97.3 |
These reported practices are high relative to other sources, such as the Nigeria Demographic and Health Survey (NPC and ICF International 2014). For example, exclusive breastfeeding was only 17 percent according to the 2013 DHS, and in another SPRING study in Kaduna state, exclusive breastfeeding was 29 percent at baseline. The fact that more than 60 percent of beneficiaries reported practicing exclusive breastfeeding1 with their latest child is encouraging and suggests that the support group approach contributed to the high levels of good practices being adopted.
Strengthening Supportive Supervision and Reporting Systems
In FY14, we developed a one-day monitoring and evaluation (M&E) training to accompany the rollout of the C-IYCF counselling package. Through this training, which was based on the generic UNICEF IYCF Monitoring and Supportive Supervision Guide, we built the capacity of 336 relevant government officials and M&E officers of OVC partners, their CSOs, MOH, and FMOWASD on appropriate documentation and data flow from the community to the national-level to strengthen the paper-based data flow within the government reporting system.
An integral aspect of IYCF counselling is supportive supervision to ensure the quality of the IYCF implementation at all levels (LGAs, PHCs, and support groups) and for all actors (OVC partners, their CSOs, community volunteers, and government partners). These supportive supervision visits are opportunities to provide technical support, reinforce key IYCF messages, and ensure that community volunteers use high-quality counselling skills in IYCF support group facilitation. We hired eight nutrition coordinators, who were responsible for overseeing the IYCF activities, including advocacy, training, and supportive supervision, in a cluster of states. Over the life of the project, we conducted 636 supportive supervision visits across the 16 implementation states. To the extent possible, we ensured that these visits were conducted in tandem with government personnel and our partners.
Improving Coordination at the National, State, and LGA Levels
Effective implementation of the F-IYCF and C-IYCF counselling packages requires close coordination and collaboration among relevant government ministries, departments, and agencies at the state and LGA levels. Across each of our implementation states, we collaborated with relevant authorities to establish nutrition focal persons meetings at the LGA level. These meetings are a platform for planning and reviewing IYCF-related activities conducted in the focal LGAs by our UGM and LOPIN partners; sharing and disseminating relevant information (such as vitamin A supplementation, growth monitoring, and hygiene); and identifying and proffering solutions to critical challenges/constraints to the effective rollout of the C-IYCF counselling package. The meetings brought together state nutrition officers, state monitoring and evaluation officers, LGA OVC desk officers, agriculture extension officers, technical/nutrition staff from the UGM and LOPIN partners and their respective CSOs, and LGA nutrition focal persons. Over the life of the project, we supported 38 of these meetings. Meetings were typically conducted on a quarterly basis once the training cascade was complete.
The coordination meetings were also to streamline activities, as implementing partners shared information about their individual projects; this also helped the government to be better equipped and focused in their own interventions. Starting in 2014, we convened the LGA nutrition focal persons in state by hosting a meeting biannually, once trainings were complete. They were a forum through which nutrition stakeholders reviewed the rollout of IYCF activities, and reinforced the strategy and the state’s expectations within each of the LGAs. Over the life of the project, we supported a total of 38 these meetings.
Improved National Social and Policy Environment for Priority Nutrition Practices and Services
Technical Support to Government of Nigeria
Our advocacy efforts at the federal, state, and LGA levels (highlighted above) included the provision of technical assistance to the GON.
- In FY13, we provided a technical review of the Nutritional Care and Support for Vulnerable Children: A Resource Manual, developed under IYCN in conjunction with the FMOWSD and other partners. The USAID-funded ASSIST project led this process, with SPRING providing technical support for the food and nutrition component to help ensure consistency in the quality of service delivery to OVC in Nigeria.
- In April 2013, we met with the FMOH to review the health management information systems (HMIS) for nutrition information. During this meeting, we identified gaps and provided several recommendations to improve the collection and analysis of nutritionrelated data. We then helped FMOH develop harmonized data collection tools for IYCF programming that can generate data at the community-level and housed in a national database. These tools are being used in the country pending revision to the National HMIS in 2017. The development of IYCF data tools was paramount in the absence of an IYCF data-capturing mechanism at the state and national levels. In collaboration with UNICEF, Save the Children, and other members of the IYCF technical working group (TWG), we supported the Federal Ministry of Health in harmonizing the several IYCF monitoring tools in use in the country. Following the completion of the harmonization of the tools, we produced copies and facilitated their distribution to all of our relevant partners: 500 copies each of the support group register; one-on-one counselling register; and C-IYCF monthly summary forms; 1,200 copies of health facility-based monthly summary forms; 100 copies of the LGA monthly summary forms; 20 state-level forms; and 5 national-level forms.
We have been welcomed as a technical partner to nutrition-related meetings chaired by either the FMOH or the Federal Ministry of Budget and Planning. We have continued to contribute to national-level nutrition coordination and policy efforts through regular participation in various national IYCF and nutrition platforms, including:
- National Complementary Feeding Strategic Planning Meeting to Accelerate Responses toward Improved Complementary Feeding of Children Ages 6–23 Months. During the meeting, SPRING presented its work and the joint SPRING-UNICEFFMOH C-IYCF counselling package evaluation. SPRING also chaired a session on strategies to improve complementary feeding.
- National Infant and Young Child Feeding Communication for Development Strategy 2016–2020—Technical Validation and Messaging Workshop. SPRING participated in the strategy development process and made significant contributions during the technical validation and messaging workshop.
- 2016 Joint Assessment of Progress Setting Exercise for Scaling up Nutrition Movement in Nigeria. We participated in the assessment process and worked in one of the four groups set up during the meeting.
- National consultative meeting in preparation for Nigeria’s attendance at the Rio 2016 Nutrition for Growth Summit.
- Strategic Review and Validation Meeting for Policy Analysis on the Adoption and Implementation of the National Strategic Plan of Action for Nutrition (NSPAN 2014–2019).
- Budget Analysis for Nutrition from 2010–2015 at national and state levels.
- Development Partners Nutrition Advocacy Group Meeting. SPRING provided project updates with emphasis on sensitization activities and advocacy to policymakers and traditional/community leaders in the states and LGAs where we work.
- 2016 Lancet Series and High Level Policy Dialogue on Breastfeeding. SPRING contributed to the development of a communique on exclusive breastfeeding.
National IYCF Technical Working Group
In FY14, SPRING began supporting the FMOH’s National Infant and Young Child Feeding Technical Working Group (IYCF TWG, also referred to as the IYCF Task Force), which works to streamline, advocate, strategize, and proffer solutions to challenges pertaining to the nutrition and health of children under five years of age in Nigeria. The group comprises government ministries and parastatals, international nongovernmental organizations, UN agencies, and other stakeholders. However, failed coordination between the FMOH and the National Food and Nutrition Committee, which lacked a secretary, led to the TWG’s inactivity. This created a vacuum that led partners to create parallel mechanisms to implement their activities. In FY14, SPRING helped reactivate the group by taking on the role of secretariat, supporting agenda creation and minutes circulation, and coordinating with the government to ensure meetings were held on a regular schedule. SPRING provided support to four of the group’s meetings over the life of the project.
Following its reactivation, the IYCF TWG led the development of the National Policy on Food and Nutrition and Plan of Action and review of the National Strategic Plan of Action for Nutrition (2014–2019). The IYCF TWG also strengthened coordination of national nutrition stakeholders by hosting meetings of the Development Partners Nutrition Advocacy Group, whose members also belong to the IYCF TWG. Theirs is a forum for information exchange and identification of key issues and joint initiatives, convening major nutrition actors, including UN agencies and nongovernmental and civil society organizations such as Civil Society for Scaling up Nutrition in Nigeria.
Enhanced Evidence Base for the CIYCF Counselling Package

In 2015, SPRING partnered with UNICEF in Nigeria and the Federal Ministry of Health to conduct an evaluation of the C-IYCF counselling package in Kaduna state. The evaluation is the first rigorous evaluation of the C-IYCF counselling package, which has been adapted for use in more than 20 countries. The findings are intended to inform national and global efforts to improve IYCFrelated programming. SPRING’s role in this evaluation is supported fully through funding from USAID/Washington, and is taking place in areas outside SPRING/Nigeria’s implementation LGAs. A final report, detailing the results of the evaluation, will be published in mid-2017.
Improved Nutrition Programming Efforts to Prevent Undernutrition in OVC Project Communities
We provided technical assistance to the wider nutrition and food security programming efforts of OVC partners and their supported CSOs. This technical assistance was requested on an ad hoc basis and included reviews of nutrition assessment tools and strategies relevant to IYCF, provision of recommendations on food-based approaches to combat undernutrition, and information on vitamin A deficiency. We also responded to two requests for training materials (see below).
Nutrition and Hygiene for Children Ages 2–17
Our LOPIN and UGM partners requested our technical assistance to help them meet the nutritional needs of the older OVC who benefit from their programs (beyond the first 1,000 days). In FY15, SPRING conducted a landscape assessment (Review of Programming for Orphans and Vulnerable Children in Nigeria) that focused on identifying current nutrition best practices among children 0–17 years of age (but particularly those between 2 and 17 years), and strategies to implement the identified practices. SPRING, in conjunction with OVC partners, then defined key nutrition messages to be incorporated in any materials developed for use by CSOs. We then created a training package for our five OVC partners to use with their local partners to reach children in this age group.
The Nutrition and Hygiene for Orphans and Vulnerable Children in Nigeria: A Training Guide for Community-Based Organisations (referred to as the Nutrition and Hygiene for OVC in Nigeria training package) builds the nutrition capacity of CSO staff and volunteers and includes activities and lesson plans to use directly with children. Our partners identified community health workers, “Kids’ Club” leaders, early childhood development (ECD) center leaders, and other community workers as the target audience for this training, because they provide support and information on nutrition and hygiene to caregivers and children (from birth through adolescence).
The OVC training package provides basic technical knowledge on the nutrition and hygiene needs beyond the first 1,000 days to children who are 2–17 years old, highlighting the needs of OVC and those living with or affected by HIV and AIDS.
In July 2016, we tested key concepts in the OVC training package in four communities in the FCT (Tungan Ashere, Jiwa, Gwagwa, and Basan Jiwa) with volunteers who work in Kids’ Clubs and ECD centers and samples of children within each age group. During the process we checked for the flow, ease of understanding, and applicability to the local Nigerian setting. For example, the training builds on the Go, Grow, Glow nutrition curriculum initially developed for use in the United States and since adapted for use in Ghana, Zambia, Tanzania, Mozambique, and other countries. We changed the concept’s terms to Move, Grow, Shine to reflect what resonates in Nigerian local contexts.
In September 2016, we conducted a pilot training of trainers using the package. We trained 26 participants from our partners (the Ministry of Education, MOH, MOWASD, Universal Basic Education Board, and state primary health care development boards) as master trainers over four days to cascade this training in their respective organizations.
Organized in a modular fashion, the nutrition and hygiene for OVC in Nigeria training package is designed for both master and cascade trainings using the appropriate age module(s) for participants. The training package includes:
- guide for facilitators,
- introductory module for all who facilitate activities with children,
- early years module for use with children 2–5 years old,
- middle years module for use with children 6–11 years old,
- adolescent years module for use with adolescents 12–17 years old, and
- job aids and handouts.
With SPRING’s support to build a pool of master trainers, each of the five OVC partners is now able to cascade the trainings across the CSOs and communities in which they work. This training is the first of its kind in Nigeria, and other organizations and government entities, including the International Community School of Abuja, Save the Children International, and the Universal Basic Education Board, have expressed interest in using or adapting the package. The DFIDfunded WINNN project has already begun adapting this package for use in northern Nigeria.
Complementary Feeding and Food Demonstration Training
In FY16, STEER and HIFASS asked SPRING to bolster and strengthen their nutrition activities and build the capacity of their CSOs and community volunteers to counsel caregivers on complementary feeding practices through a food demonstration training. We adapted the WINNN project’s complementary feeding training to include recipes with foods available in the communities of Cross River state.
These materials can be used by health service providers, households, and communities to improve understanding and knowledge of complementary feeding. The training also emphasizes best practices around water, sanitation, and hygiene in addition to food safety during the processing and preparation of food. The Nigeria: Complementary Feeding and Food Demonstration Training Package includes:
- facilitator guide,
- complementary feeding manual,
- food demonstration manual,
- training handouts,
- PowerPoint slides, and
- recipe cards.
SPRING used this adapted training package to conduct two complementary feeding and food demonstration workshops for a total of 60 trainers in Cross River state. Participants included coordinators of focal PHCs; LGA nutrition focal persons; relevant officials from state ministries (MOH, MOA, MOWASD), program staff from STEER, HIFASS, and their respective CSO partners; and selected community volunteers.
Best Practices, Challenges, and Recommendations
Best Practices
Increasing community members' understanding of the causes and consequences of malnutrition in communities and households is key to promoting uptake of appropriate IYCF practices in Nigeria. Findings from interactions with caregivers during the IYCF support group meetings indicated that many caregivers had limited understanding of malnutrition and misconceptions about its causes. Our findings also revealed that infant feeding practices in many rural/semirural communities were heavily steeped in cultural and traditional practices. However, community volunteer activities such as home visits and one-on-one counselling effectively promoted the adoption of appropriate infant feeding practices. Additionally, we found that involving fathers and mothers-in-law in support groups encouraged mothers to adopt optimal IYCF practices, and installing male support group facilitators in communities located in the northern states, where society is more patriarchal, convinced men to allow their wives to join support groups.
Changing behavior is not a linear process and requires a sustained effort because results are not immediately visible. We consider it a best practice to invest significant effort in gaining buy-in at the state, LGA, and community levels early. Advocacy and sensitization meetings with all relevant stakeholders/policymakers at national level, state, and LGA levels should continue to encourage resource commitment for nutrition activities and interventions that target the first 1,000 days. Our sensitization meetings showcased SPRING activities and enhanced our ability to promote dialogue and influence policy on the effective implementation of the IYCF counselling package. At these meetings, our government partners were highly appreciative of our efforts and commended us on our achievements. In one case, our advocacy efforts resulted in the allocation of 1 million Naira to nutrition in the 2016 budget by the Jos South local government (see the success story Allocating Money for Better Nutrition in Nigeria in Annex 2).
Having a set of training materials that are adapted to the local context and are technically sound is important because trainings focus on building an individual’s knowledge and his/her interpersonal skills (counselling and negotiation). Refresher and catch-up trainings should be considered to ensure that these skills stay sharp and to prevent gaps in trained personnel (due to attrition or transfer).
Rolling out the IYCF counselling packages goes beyond training, and the majority of effort is spent on follow up visits to ensure the quality of IYCF messages and counselling. Ensuring that resources are available (staff level of effort, transportation, etc.) to conduct this aspect of implementation is critical to its success and the creation of behavior change. For sustained quality of the IYCF counselling, quality improvement approaches that address broader nutrition-specific interventions within the Nigerian health system are necessary. Strengthening supportive supervision, mentoring, and coaching techniques is important for maximum impact, and other innovative approaches should be explored.
Challenges and Recommendations
SPRING ended program activities on September 30, 2016. Over the life of the project, we faced a number of obstacles and challenges that impacted our implementation, including political instability resulting from national and local elections, strikes by government workers due to nonpayment of salaries, and sectarian violence and insecurity across many of our implementation states. Heavy rainfalls causing severe flooding made some LGAs inaccessible, preventing planned supportive supervision activities.
We also faced challenges in the harmonization and coordination of activities with OVC partners during the work plan development process. Additionally, some of our partners took a long time to select the LGAs in which they would work. Both of these instances delayed our ability to implement trainings and then conduct supportive supervision. Defining the roles and responsibilities of partners is important to avoid delays and misunderstandings, and the agreements made in planning meetings should be respected.
Nutrition officials at state and LGA levels have the capacity to provide supportive supervision to facilities and communities, but limited government funding makes it difficult to conduct routine supervision. It is important that funds for supportive supervision of facility and community IYCF counselling are included in state and LGA operational plans and budget forecasts.
The Ministry of Health at national and state levels, in collaboration with the Ministry of Education at national and state levels, should institutionalize a system for updating nutrition technical information (such as found in the F-IYCF and C-IYCF counselling packages) in the preservice training curriculum for allied health professionals and as part of in-service health training at institutions.
While SPRING’s work focused on promoting optimal IYCF practices almost exclusively, we recommend educating stakeholders to use a multi-sectorial approach to raise communities’ understanding of the multiple causes of malnutrition and mobilize them to prevent and subvert malnutrition. Given our experience working with adolescents and children over 2 years of age, we also recommend expanding beyond the first 1,000 days to promote good nutrition and hygiene practices throughout the life cycle, which can contribute to a healthy pregnancy. The adoption of optimal nutrition practices at a younger age can lead to sustained behavior change.
Conclusion
Over the course of five years, we have built the capacity of government, PEPFAR-funded partners, CSOs, and communities across 16 states and 122 LGAs, covering all six geopolitical zones of the country. The results of our capacity and beneficiary assessment have demonstrated that it is possible to work at scale without compromising the quality of implementation. Over 70 percent of CSOs, health workers, and community volunteers who were trained by SPRING over the course of the project retained high levels of knowledge on IYCF. More than 80 percent had favorable attitudes toward issues such as male involvement in support groups and in the home, women’s and children’s nutrition when the mother is HIV-positive, and breastfeeding among working women. Most offered favorable opinions and comments, excerpted below, about support from SPRING and partners. The capacity built by SPRING appears to have led to high quality program implementation, which has resulted in positive IYCF practices among support group beneficiaries.
To a large extent SPRING has improved the knowledge of people on breastfeeding and complementary feeding. Prior to SPRING program people’s knowledge on infants and children feeding is very low but now from the support from SPRING people now know how address the breastfeeding difficulties and give their children breastfeeding.
-OVC desk officer
SPRING training and support has transformed in our LGA by the strategy of IYCF support group, this has really changed their belief on young feeding, most of our caregivers now know the importance [and have] changed from the misconception of breastfeeding.
-Nutrition focal person
With SPRING support, integration of nutrition into OVC programming was a success; we now use the caregiver’s forum to spread IYCF messages.
-CSO staff person
SPRING training has helped me to integrate IYCF messages in the ANC service for the benefit of pregnant women and as such more pregnant women are accessing the clinic than before.
-Primary health care provider
Prior to SPRING training, I was someone who did not agree with exclusive breastfeeding, but now I have full information about the benefits, I now share the message to the women in my community and they are adopting it. This is because I attended the training and I’m impacting the knowledge on my community members.
-Community volunteer
SPRING found that improving maternal and child nutrition practices by promoting optimal IYCF behaviors can be achieved with investments in capacity building, especially for community volunteers and facility-based health workers. The majority of our training participants were enthusiastic and appreciative of the opportunity to learn and practice counselling skills. Many of those trained have gone on to build the capacity of other community- and facility-based health workers. This cascade approach has significantly raised awareness of appropriate IYCF practices in focal communities, and concurrently increased adoption of optimal practices by caregivers and their families. The development of a training package for IYCF for children 2–17 years old provides an opportunity for partners to move beyond the first 1,000 days and influence the nutrition and hygiene behaviors of children, particularly OVCs, from an early age.

To view the annex, please download the full report above.
Footnotes
1 Note that the DHS and SPRING’s assessment measured exclusive breastfeeding differently. Although the data is not exactly comparable, the difference suggests that the training and IYCF support group methodology has had a positive effect.
References
Bhutta, Z., Das, J., Rizvi, A., et al. 2013. “Evidence-based Interventions for Improvement of Maternal and Child Nutrition: What Can Be Done and At What Cost?” The Lancet 382: 452– 77.
National Population Commission (NPC) [Nigeria] and ICF International. 2014. Nigeria Demographic and Health Survey 2013. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International.
Federal Ministry of Women’s Affairs and Social Development. 2008. Key Findings from the 2008 Situation Assessment and Analysis on OVC in Nigeria. Abuja, Nigeria: Federal Ministry of Women’s Affairs and Social Development.
FMOH (Federal Ministry of Health–Nigeria). 2013. National HIV and AIDS and Reproductive Health Survey, 2012 (NARHS Plus). Abuja, Nigeria: Federal Ministry of Health.
UNAIDS (Joint United Nations Programme on HIV/AIDS). 2013. Global Report: UNAIDS Report on the Global AIDS Epidemic, 2013. Geneva: UNAIDS.
UNICEF (United Nation’s Children Fund). 2006. The State of the World’s Children 2007: Women and Children. The Double Dividend of Gender Equity. New York, NY: UNICEF.



