The SPRING/Digital Green Experience in Niger
Evidence from a Community Video Approach for Nutrition and Hygiene Behaviors

Located in the Sahel, Niger is characterized by harsh climate conditions that contribute to structural food crises and high rates of severe acute malnutrition among children. The people of Niger have experienced frequent shocks, such as conflict, drought, and food shortages, which will likely worsen as a result of climate change and expanding population. With 43.9 percent of children under five years stunted, the country needs to introduce approaches that produce rapid results. Addressing the nutrition, health, and livelihoods needs of communities in Niger requires a rapid and flexible communication approach that can be adapted to contextual needs at the community level. Funded by the U.S. Agency for International Development (USAID), SPRING is a five-year project committed to reducing anemia and stunting among women and young children through the expansion of effective social and behavior change communication (SBCC) and nutrition-sensitive programs at scale.
Following a successful collaboration in India, SPRING and Digital Green (DG) have built partnerships with existing community groups and introduced an innovative community media approach in Niger. The SPRING/DG pilot intervention in Niger aims to contribute to a decrease in childhood illnesses caused by poor handwashing, and to support improved dietary intake through an increase in the use of responsive feeding practices. The approach enables rural communities to create and share videos that promote high-impact maternal, infant, and young child nutrition (MIYCN) and hygiene behaviors. This report presents results from a mixed-methods evaluation on the acceptability, effectiveness, and scalability of the SPRING and DG community-led video approach on MIYCN and hygiene behaviors in Niger.
Research Questions
The evaluation seeks to answer the following research questions:
- What were the experiences and perspectives of participating beneficiaries and mediators in terms of the acceptability of the community video program? How feasible did they find implementation?
- What was the effect of the SPRING/DG approach in terms of changing knowledge, attitudes, and adoption of handwashing and responsive feeding behaviors in the target group? Did knowledge and behavior adoption diminish/increase over time?
- What is the cost per adoption of behavior and cost per person reached in the SPRING/DG pilot intervention areas? What is the cost of scaling up the intervention to new communities or introducing new videos?
Methods
Our evaluation applied a mixed-methods study design. Quantitative cross-sectional surveys measured the effectiveness of the interventions and were administered at three time periods: prior to video exposure (baseline), four to eight weeks following video exposure (second survey), and three to four months following video exposure (endline) to test sustainability of adoption. Focus group discussions (FGDs) assessed acceptability, as well as the potential to scale up and sustain the intervention. We collected cost data to determine the cost per beneficiary reached and behavior changed as well as to determine what resources would be required to scale up the intervention.
Results
Feasibility and Acceptability of the Community Video Approach
Findings from the FGDs were promising and indicated that community members, including women of reproductive age (WRA), men, and adolescents, perceived the community video approach was an acceptable and feasible tool to support behavior change. Program beneficiaries noted that the scheduling and duration of the video viewing were appropriate. However, due to the high levels of interest, at times the viewing area became hot and crowded and there were not enough places to sit. Overall, women felt a connection to the stories shared and felt that the visual presentation helped facilitate an understanding of the messages beyond what had previously been shared verbally. Findings from the FGDs also indicated that the videos had generated excitement that was translating into changes in social norms. Pilot intervention beneficiaries and mediators found that participation in the activities helped to elevate their social status, with other community members consulting them about the messages shared through the videos and home visits.
Pilot intervention beneficiaries and mediators also acknowledged the importance of the home visits, stating that the visits helped to reinforce the understanding of messages shared during the video viewing and also offered an opportunity to share the information with influencers in the household, including husbands and mothers-in-law. Women also noted that the pilot intervention’s emphasis on inviting influencers to the video viewings was helpful since this provided the women with additional support in convincing household members who may be resistant to behavior change.
Effectiveness of the Community Video Approach
Findings from the quantitative surveys indicated that the community video approach was an effective tool for achieving MIYCN behavior change as shown in tables 1 and 2. Survey findings indicate that use of the community video approach significantly increased the presence of a handwashing station at home (as demonstrated in the videos) from 14 percent at baseline to 59 percent one to two months after the video was shown. In addition, the percentage of households with a handwashing station with soap and water, indicating regular use, increased significantly from 73.8 percent to 96.2 percent.
Findings for the second priority behavior studied, responsive feeding of children 6–24 months and feeding from a separate plate, also indicate very promising results. After watching the video, the percentage of children within arm’s reach of a responsible person at the last meal increased significantly from 65 percent to 80 percent. The percentage of women who fed their child from a separate plate increased significantly from 70 percent to 97 percent.
Table 1: Change in Handwashing Behaviors before and after Video Viewing
| Baseline (April 2015) | 1–2 Months after Video Exposure (June 2015) | 3–4 Months after Video Exposure (August 2015) | |
|---|---|---|---|
| Households with at least one place designated to wash hands | 14% | 48.8% | 59% |
| Total number | 301 | 322 | 356 |
| Households with a handwashing station with soap and water | 73.8% | 95.5% | 96.2% |
| Total number | 42 | 157 | 210 |
Table 2: Change in Responsive Feeding and Feeding from a Separate Dish Behavior before and after Video Viewing
| Baseline (April 2015) | 1–2 Months after Video Exposure (June 2015) | 3–4 Months after Video Exposure (August 2015) | |
|---|---|---|---|
| Total number | 301 | 322 | 356 |
| Percentage of women who said a responsible person helped the child at the last meal | 87.7 | 94.7 | 92.7 |
| Percentage of women who have a separate plate for their child | 69.8 | 89.1 | 96.6 |
| Percentage of women who said child was less than an arm’s length from a responsible person at the last meal | 64.5 | 76.7 | 79.5 |
| Percentage of women who actively encourage their child to eat (based on encouragement scale) | 31.2 | 70.2 | 85.1 |
Cost of Implementing the Community Video Approach
Our analysis determined the cost per beneficiary reached to be approximately US$16.19 per person. Based on the numbers of beneficiaries whose behaviors changed, we determined the cost per handwashing adoption of behavior changed to be US$28.91 per beneficiary and US$36.24 per beneficiary who “adopted” the behavior of maintaining a separate plate for the child. Cost estimates for scale-up included a small stipend increase for the project mediators and were extrapolated for two scenarios to determine the added costs associated with expanding the intervention from 1,500 beneficiaries to 7,500 beneficiaries. Using the existing 10 videos produced by the proof of concept, we estimated the cost to scale up the program at US$277,169. As a result, the cost per beneficiary fell to US$3.73 per person reached, US$6.60 for per handwashing station behavior changed, and US$8.27 for the separate plate behavior changed. A second scenario estimated the costs of expanding the intervention to 7,500 beneficiaries and producing new video content. The costs associated with the second scenario were US$304,887. As a result, the cost per beneficiary would be US$4.13 per person reached, US$7.26 for the handwashing station behavior changed, and US$9.10 for the separate plate behavior changed.
Conclusion
The SPRING/DG collaboration in Niger shows that the approach can be implemented successfully in the resilience context of Niger. Results from the mixed-methods evaluation highlight the potential of the community video approach as an innovative and effective approach for fostering both social and individual nutrition and hygiene-related behavior change. Overall, evaluation results show that using multiple channels for disseminating messages and engaging with key influencers is a promising approach to empower women, men, and communities to improve their health through improved nutrition and hygiene behaviors.
Introduction
Niger, located in the Sahel, is characterized by harsh climate conditions that contribute to structural food crises and high rates of severe acute malnutrition among children. In 2012, the under-five mortality rate was 127 per 1,000 live births and 43.9 percent of children under five years were stunted1 (INS and ICF International 2012). A number of factors contribute to the high levels of child deaths and malnutrition, including childhood illness and inadequate dietary intake. Underlying determinants to these immediate causes include household food insecurity, poor child care practices, insufficient health services, and an unhealthy environment (Black et al. 2008). Many of these underlying determinants are influenced by cultural norms and practices, including polygamy, an emphasis on male decision making, and low levels of literacy (Moreaux 2015).
The World Health Organization (WHO) recommends a number of interventions, including handwashing with soap at critical times (after toilet use and before the preparation of food), as means of preventing diarrheal diseases, which contribute to nutritional deficiencies, reduced resistance to infections, and impaired growth and development (WHO 2015). There is also an increasing recognition that feeding behaviors and styles can influence complementary feeding outcomes and dietary intake and thus the growth of infants and young children (IYC) (Bentley, Wasser, and Creed-Kanashiro 2011). Promoting practices that support appropriate feeding behaviors and styles as well as hygiene requires highly contextualized social and behavior change communication (SBCC) strategies that address the constraints presented in rural, traditional, resource-constrained societies such as Niger.

SBCC is uniquely challenging in highly remote areas. Rural populations can be difficult to engage with as a result of poor infrastructure and limited access to health care, thereby making it challenging for health workers to reach those most in need. Mass media approaches require access to radio or television, which may not always be available in rural environments. In Niger, fewer than 50 percent of households in rural areas own a radio and only 3 percent in rural areas own a television (INS eand ICF International 2012). In addition, information often flows outward through mass media in one direction from urban centers, where a small group of people and interests determines which information rural communities should receive, rather than tailoring media content based on an exchange of ideas and requests that allows adaptation of information to the needs of rural communities (Berrigan 1979).
The use of video as a SBCC medium offers several advantages when working in rural communities, such as more standardized content with fewer inconsistencies across educators and high receptivity and understanding among low-literacy populations. Behavior change approaches that incorporate videos coupled with guided discussions at the community level have shown promise in public health (Desta et al. 2014; Khoury et al. 2002; Roye and Hudson, 2003; Tuong, Larsen, and Armstrong 2014). However, evidence is limited on the use of community videos specifically to support MIYCN and hygiene behaviors.
Following a successful collaboration in India, SPRING and Digital Green (DG) have built partnerships with existing community groups and introduced an innovative community media approach in Niger (Kadiyala et al. 2014). The goal of the SPRING/DG pilot intervention in Niger is to contribute to a decrease in childhood illnesses caused by poor handwashing, and to support improved dietary intake through an increase in the use of responsive feeding practices. This report presents findings from a mixed-methods evaluation to assess the acceptability and effectiveness of implementing the community video approach to address MIYCN and hygiene behaviors in a resource-constrained setting such as Niger. The study further explores the factors influencing the potential to scale up the intervention and sustain activities.
Description of the Intervention
Supported by USAID, the SPRING project in collaboration with DG implemented a pilot intervention from late 2014 through 2015 to test the use of facilitated community video for the promotion of high-impact MIYCN and hygiene behaviors in the resilience context of Niger. We adapted the approach from the SPRING/DG collaborative approach, implemented in India 2012. We worked in partnership with three projects: the Resilience and Economic Growth in the Sahel–Enhanced Resilience Program (REGIS-ER), and two Food for Peace projects, the Livelihoods, Agriculture and Health Interventions in Action (LAHIA) and Sawki projects, which are led, respectively, by the National Cooperative Business Association CLUSA International (NCBA CLUSA), Save the Children, and Mercy Corps. We collaborated with the partners to test the community video approach in their respective intervention villages. We began implementation in January 2015, first identifying 20 villages: 15 in the commune of Guidan Roumdji under REGIS-ER and Sawki, and five villages in the commune of Aguie under Save the Children. Both communes are in the region of Maradi, with its capital—Maradi town—located 670 kilometers from Niamey. The selected communes are situated approximately one hour’s driving distance from Maradi town.
Over the implementation period, our pilot intervention team worked with select communities to develop and disseminate videos focused on 10 MIYCN and hygiene themes. Members from select communities performed as actors, or “stars,” in the videos, which our mediators then presented during monthly community meetings, accompanied by facilitated discussions, of four existing community groups2 established by the implementing partner projects. The videos focused on a number of key themes, such as dietary diversity, handwashing, exclusive breastfeeding, and complementary feeding practices, including responsive feeding of young children using a separate dish. In addition to disseminations to the four existing community groups, our mediators screened videos for four groups of influencers, including mothers-in-law, husbands, and co-wives. Core group members selected these influencers on a per-video basis, to help facilitate their adoption of the promoted behaviors at home. We encouraged core group members to choose different influencers for each video depending on the theme and who they felt would benefit from seeing the video. Field mediators (or volunteers) shared the videos, led interactive discussions following the videos, and conducted home visits to address any questions raised by participants and check whether group members actually understood the practice correctly, or promoted the practice to others in their family or community.
Over the course of implementation, the pilot intervention reached 1,644 primary group members (1,278 women and 366 men) through 80 community video screenings. For each video, the process involved adapting the steps outlined and the tools provided in SPRING’s Community Video for Nutrition Guide as shown in Figure 1. Because of the evaluation time frame, the study focused on behaviors that could be adopted immediately following video exposure. For this reason, we selected for study handwashing and responsive feeding behaviors.
Figure 1. Community Video for Nutrition Guide Steps

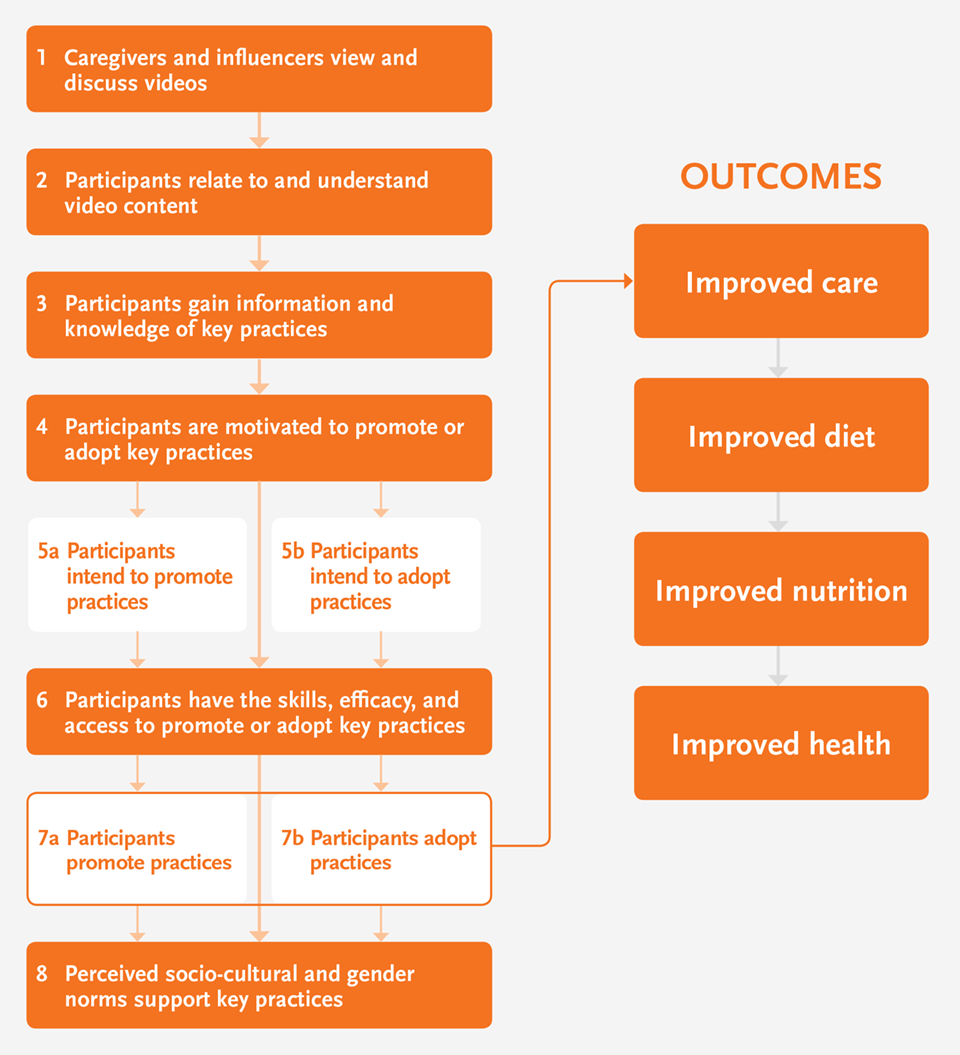
Conceptual Framework
The SPRING/DG intervention is guided by Bandura’s social learning behavior change model and the socioecological model (Bandura 2004; Stokols 1996). Both theories acknowledge the need to introduce interventions that address cognitive, behavioral, and environmental factors influencing behavior change. The conceptual framework presented in Figure 2 summarizes the pathway of change the SPRING/DG intervention seeks to facilitate to ultimately contribute to improvements in handwashing and responsive feeding behaviors. To address cognitive factors, the intervention focuses on sharing information that supports improved knowledge on and attitudes toward on the behaviors. To address behavioral factors, the videos provide demonstrations of the behavior by actual community members, thereby proving that viewers can develop self-efficacy to practice the behaviors. Finally, by providing the members of women’s groups with the option to invite their influencers to video screenings, the intervention addresses environmental factors, including social norms, that are important determinants in the Niger context, where women have limited decision-making power. The social learning theory proposes that improved knowledge, attitudes, and increased self-efficacy can ultimately result in behavior change.
Figure 2. SPRING/DG Niger Proof of Concept Conceptual Framework
The mixed-methods evaluation aims to determine the acceptability and effectiveness of implementing the community video approach as well as understand the factors that will influence scale-up and sustainability, by answering the following questions:
- What were the experiences and perspectives of the beneficiaries and mediators in terms of the acceptability of the community video program? How feasible did they find implementation?
- What was the effect of the SPRING/DG approach in terms of changing knowledge, attitudes, and adoption of handwashing and responsive feeding behaviors in the target group? Did knowledge and behavior adoption diminish/increase over time?
- What is the cost per adoption of behavior and cost per person reached in the SPRING/DG pilot intervention area? What is the cost of scaling up the intervention to new communities or introducing new videos? What other factors should be considered when scaling up the intervention?
Methods
We applied a mixed-methods study design. Quantitative surveys measured the effectiveness of the interventions and were administered at three time periods: prior to video exposure (baseline), four to eight weeks following video exposure (second survey), and three to four months following video exposure (endline) to test sustainability of adoption. Focus group discussions (FGDs) assessed the acceptability, and potential to scale up and sustain the intervention. We collected cost data to determine the cost per beneficiary reached and behavior changed as well as to determine what resources would be required to scale up the intervention.
Qualitative Study
The objectives of the qualitative research were to address questions on the acceptability of the pilot intervention, and to gather feedback on the implementation to inform scale up by interviewing program beneficiaries and mediators. To facilitate partner buy-in and increase program learning, we held FGDs and in-depth interviews (IDIs) during a one-week stakeholder workshop led by program implementers, technical advisors, and researchers in Maradi, Niger, in August 2015. We held two rounds of FGDs with both program beneficiaries and mediators, for a total of 14 FGDs. The first round of FGDs focused on the video screening experience and the second round focused on the home visit experience. Specific themes explored in the FGDs included:
- Acceptability of the video schedule and viewing environment
- Comprehension of video messages by group members
- Effect of video on group participation and social status
- Effect of video on influencers invited to attend
- Home visit experience
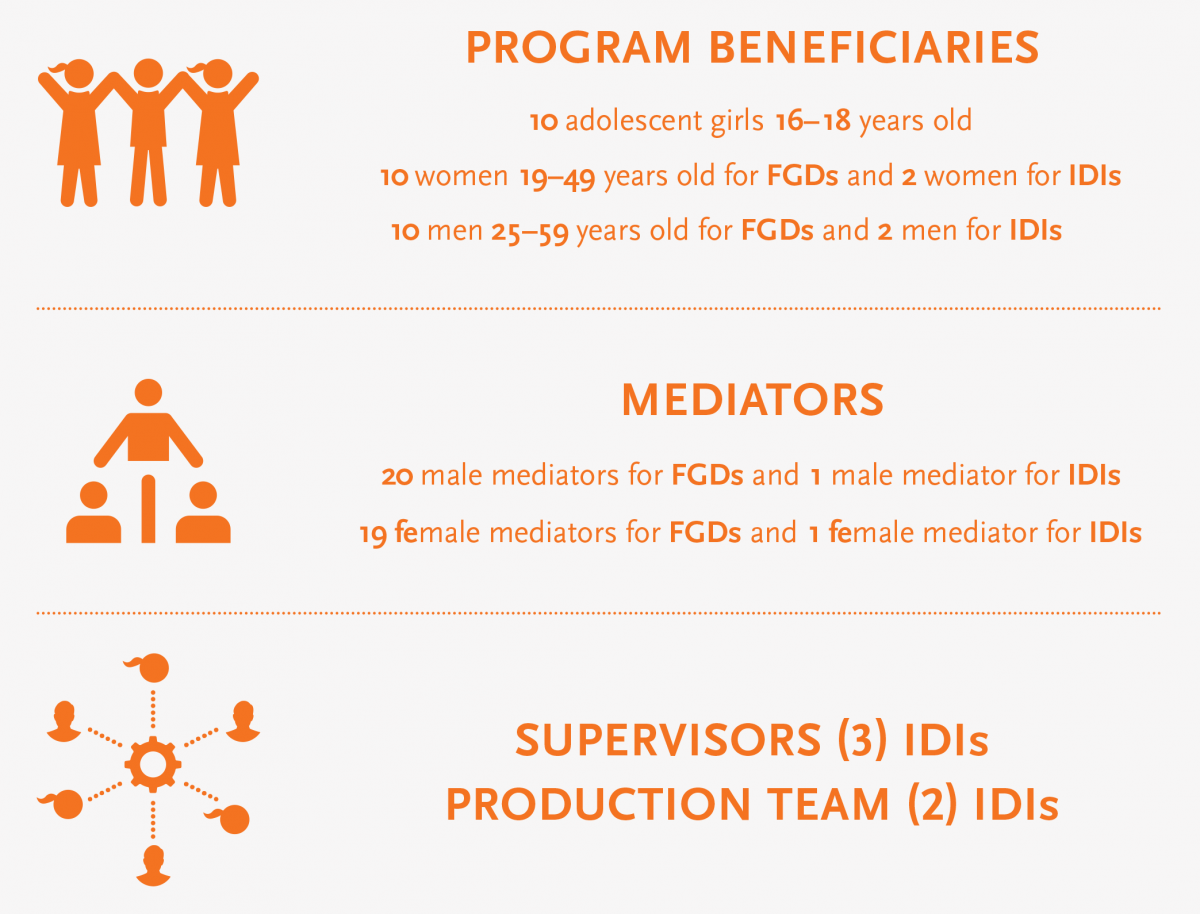
We selected a total of 33 respondents from the four existing community groups. The respondents were purposively selected to represent a mix of groups and partners participating in the pilot intervention (see Figure 3). We invited all 40 mediators assigned to the pilot intervention to participate in the workshop, and a total of 20 male mediators and 19 female mediators were able to attend. IDIs were conducted with one male and female mediator and two male and two female beneficiaries, two members of the production team, and all three supervisors involved in the program. The interviews were conducted in Hausa with permission from respondents, recorded using a digital audio recorder, transcribed into French, and coded in MS Word. We applied thematic analysis techniques to identify themes and document key activities.
Figure 3. Description of Qualitative Research Respondents
Quantitative Study
The objectives of the quantitative surveys were to measure the effectiveness of the interventions and assess the prospects for sustainability by understanding the acceptability and perspective of the program beneficiaries. We administered three rounds of cross-sectional surveys to women of reproductive age (WRA) (15–49 years) with a child between the ages of 6 and 23 months, who were invited to participate in the video viewing. We administered the surveys at three time periods: prior to video exposure (baseline), four to eight weeks following video exposure (second survey), and three to four months following video exposure (endline) to examine short- and long-term effects of exposure. In total, we interviewed 301 eligible women at baseline, 322 women at the second survey, and 356 women at endline. The numbers of women interviewed increased slightly over time because we included women interviewed at baseline as well as women whose child entered the 6–23-month age range over the study period. Some women were repeatedly interviewed over time, but the cohort was not equivalent at each time point as some new women were added at each.
We selected respondents from a list of project participants provided by the lead partner in each village. The project list did not include information on age and whether the respondent had a child between 6 and 23 months, so eligibility was determined at the time of the interview. Interviewers approached each household where a project participant lived and requested to speak with the project participant, who agreed to participate in the survey by oral consent. We collected basic information, including age and date of last birth to determine eligibility. When a participant was determined eligible, the data collector proceeded to administer the survey. The survey was administered by trained interviewers in Hausa and entered in French using mobile phones. Encrypted data were transmitted to SurveyCTO’s server and downloaded for cleaning. Queries were returned to field supervisors. The supervisors then worked with data collectors to respond to queries and address any errors or inconsistencies.
The surveys collected information on knowledge, attitudes, self-efficacy, and behaviors related to handwashing and responsive feeding. Indicators assessing behaviors were self-reported except where indicated below.
Handwashing
- Percentage of households with at least one place designated to wash hands (observed by interviewer)
- Percentage of households with handwashing station near the latrine or kitchen (observed by interviewer)
- Percentage of households with handwashing station with soap and water (observed by interviewer)
- Percentage of handwashing stations maintained by the husband
Responsive Feeding
- Percentage of women who said child was helped by a responsible person at the last meal
- Percentage of women who said that the person responsible for helping the child was less than an arm’s length away
- Percentage of women who fed child with a separate plate for each meal
- Percentage of women who actively encouraged their child to eat
Data were cleaned and analyzed using Stata 13. Differences in knowledge, attitudes, and practices by survey round were assessed through bivariate analyses. Additional tests using logistic regressions were used to assess a subset of indicators described above by survey round while controlling for key demographic characteristics. Sociodemographic control variables in the handwashing models included age of the woman, parity, and educational attainment. Sociodemographic control variables in the responsive feeding outcome models included age of the mother, parity, educational attainment, and age and gender of the child.
Costing Analysis
We collected data to calculate the detailed costs of the intervention, including the cost per person reached and the cost per adoption of the key behaviors promoted as well as to determine costs associated with scaling up the intervention for future activities. Information was first collected to document the entire implementation process by describing all cost heads and activities. This information on the implementation process was then used to prepare the structure of the theoretical allocation tables with the definition of direct and indirect process costs, fixed, and variable costs. All partners conducted interviews with operational staff to collect cost information and data were entered and analyzed in MS Excel. Cost data, including labor, equipment, activities, and travel, were collected through interviews and crosschecked with budgets and by random audit.
Strengths and Limitations
The main strength of the methodology is that it employed both qualitative and quantitative methods. The quantitative component provided information on the extent to which behavior change occurred and the qualitative component provided information on the feasibility of introducing the intervention and evidence on how the change occurred. This helped to triangulate data and verify the survey findings through the qualitative interviews. The three rounds of quantitative surveys provided an opportunity to assess the immediate effects of the intervention as well as the potential for sustained behavior change. The study has a number of methodological limitations. First, the study lacks a comparison group, which limits the ability to determine if factors outside the intervention may have influenced study outcomes. The survey selected respondents based on their participation in existing community groups and therefore may not represent the wider population. The timing of the third survey occurred during a peak agricultural season, which may account for why some of the behavioral responses varied if household members had less time to focus on the behaviors.
Ethical Approval
Ethical approval was not required in Niger. However, the Direction Régionale de Santé Publique was notified of the study in a formal meeting. The study protocol and questionnaire were reviewed and approved by the John Snow, Inc., institutional review board based in Boston, Massachusetts. Free and informed consent of all respondents was obtained; this consent was taken in verbal rather than written form, given high rates of non-literacy in the Maradi region of Niger.
Results
In the following section, we present results by research question. First, we present results from the qualitative research on the acceptability and feasibility of the community video program. Next, we present a quantitative assessment of the effects of the intervention on knowledge, attitude, and adoption of handwashing and responsive feeding behaviors in the target group. Finally, we discuss the cost per adoption and cost per person reached in the SPRING/DG project area, with additional information on the costs for scaling up the intervention and an analysis of factors to consider when scaling up the activities.
Feasibility and Acceptability of Implementing the Approach
The section that follows presents results from the qualitative research, which seeks to understand the experiences and perspectives on the feasibility and acceptability of the community video pilot intervention.
Acceptability of the Video Schedule and Viewing Environment
During the qualitative surveys, interviewers asked beneficiaries and mediators to comment on the feasibility and acceptability of introducing the local videos in their communities. Beneficiaries and mediators spoke favorably regarding the introduction of the videos and mentioned that the scheduling and duration of the videos was appropriate and did not interfere with the beneficiary’s responsibilities.
Those interviewed raised some concerns with regard to the location and setup of the video screenings. Many beneficiaries and mediators noted that the rooms where the videos were projected were often too small for the number of people attending. This was especially the case when additional people attended the screenings. As a result, the rooms became too hot and there were not enough mats or places to sit comfortably. Several mediators recommended that venues, mats, tables, chairs, and benches be purchased or rented to create a more comfortable viewing environment in the future.
Comprehension of Video Messages by Group Members
Many women noted that they felt a connection with the stories presented in the videos and that the content reflected the behaviors and conditions common to their lives. A number of mediators and supervisors agreed that the videos were culturally appropriate, commenting that viewers appreciated the use of the Hausa language and as well as community members as actors.
The women are very enthusiastic because the actors are villagers like them and speak Hausa. This has had a great effect and resulted in significant behavior change.
—Female mediator
Some women also felt that the behaviors simulated visually in the videos were easier to understand than listening to facilitators presenting the information verbally.
It is important to project the videos during all the group meetings. The simulations conducted during the videos are easier to understand than listening to the group facilitator.
—Female beneficiary
Some misunderstandings occurred within the community regarding the videos but these were quickly resolved. For example, in one village, a chief complained that the mediator presented videos that encouraged women to stop having children. However, after the village chief participated in one of the video screenings, he realized he was mistaken and then encouraged women to attend.
Overall, feedback from the beneficiaries suggests that the videos have generated excitement within their groups and that the enthusiasm is spilling over to community members. As a result, there is evidence of greater social capital and cohesion, leading to changing social norms.
The video gave us the final push to change. I already knew many things before through my husband’s school, but it took us seeing the video to make a change.
—Female beneficiary
Here in Karazome, we have seen a lot of changes in our group. We are noting that the group is more united socially and even between us and our husbands, there is greater understanding. This is total cohesion.
—Female beneficiary
Effects of Video on Group Participation and Social Status
Some women felt that use of the videos in their existing group meetings had resulted in more frequent meetings with greater group participation. Some beneficiaries and mediators noted that their attendance at the video screenings had increased their social influence in the community.
We are considered teachers and we are given great importance. We are valued in the community because of this work; it has changed our status. We are perceived as officers to accompany and support people to change their behavior.
—Mediator
Women who watch the videos have become more informed and share their expertise with others. Meetings become more animated, some cohesion between group members is shown, and there is the birth of a spirit of competition, especially among women.
—Mediator
Effects of Videos on Influencers Invited to Attend the Videos
Mediators also asked beneficiaries to invite another person of their choice to attend a video screening. The idea was that each group member would invite a person who could influence their adoption of the behaviors promoted in the video. Many women felt that everyone should see the videos, especially their husbands, so that they would understand the meaning and encourage the women’s attendance at the health facility. The people the women most frequently invited were members of the family (mother, husband, sister, and friend) and other community leaders, even people from neighboring villages.
I invited my pregnant friend to watch the video on the one thousand days. She appreciated the video and applied the messages that she learned to support the proper development of her pregnancy.
—Female beneficiary
Inviting influencers to the video screenings helped educate others on the health topics covered, which could help influence adoption at the household level. For example, after viewing the handwashing video, women were able to come home and ask their husbands to put in place a handwashing station. Several respondents noted that when men see the videos, they understand more readily what they need to do to help their wives adopt appropriate health practices.
The men now accept letting their wives visit the health center and at times accompany them. In addition, they agree to provide money for consultations more frequently.
—Female beneficiary
The children now approach men with their bowl to request something to eat or to get help washing their hands before eating. The education has helped to connect men with their children in the sense that even men who are closed in spirit are obligated to open up and ensure that the child eats, especially when the mother is absent.
—Female beneficiary
While engaging men in the video disseminations and discussions is important, mediators mentioned that working with male beneficiaries was more challenging, particularly since certain men thought that they understood content better than the mediators. They did not see the content directly affecting their lives and their responsibilities did not always permit them to meet easily. However, mediators felt this situation could be overcome with continued education and opportunities for the men to view the videos. Also, both male and female beneficiaries thought it was very important for men to continue to view the videos.
Home Visit Experience
Home visits were meant as a means for data collection, but also provided an important opportunity for the mediators to have more focused time for explaining the messages from the video to the beneficiaries and engaging with other members of the family. However, many beneficiaries commented that they would like more frequent visits. According to the mediators and beneficiaries, the home visits helped with knowledge acquisition but also with behavior change, because the mediator’s direct engagement with the beneficiary ensured that the new information would be internalized and practiced.
The home visits have also had an effect on how families, friends, and community members speak about the topics presented in the video. When the mediator visits the family, they address not only the beneficiary but also the entire family, which helps to spread the information throughout the family and obtain their support.
According to adolescent beneficiaries, families, friends, and community members were more favorable to the subjects brought up in the videos during the home visits, and the home visits provided a certain level of credibility to those who attended the meetings. The visits helped improve the transmission of messages.
The family knows that the group members are not lying and they feel the information interests them and gives them a certain pride in the community.
—Adolescent beneficiary
However, some mediators said the presence of family members at times made the home visits less effective; in some cases a female beneficiary did not feel comfortable expressing her concerns in the presence of parents or in-laws.
Many beneficiaries felt that the home visits should continue after the pilot intervention concluded. Specifically, the women mentioned the need to reinforce the messages shared through the video screenings, the importance of sharing the information with other members of the household, and the need for support with the behavior adoption.
Effectiveness of the Community Video Approach on Handwashing and Responsive Feeding Behaviors
The following section presents results from the quantitative surveys, which assessed the effect of the SPRING/DG approach on knowledge, attitudes, and adoption of handwashing and responsive feeding behaviors.
Handwashing Behaviors
Figure 4 presents knowledge, attitudes, self-efficacy, and self-reported/observed behavior related to the presence of a handwashing station (i.e., tippy tap3) in the household. As shown in Figure 4, knowledge of the need to have a handwashing station among women of reproductive age who had a child in the two years preceding the survey was high at baseline and increased slightly throughout the pilot intervention, from 94.4 percent at baseline to 97.2 percent at endline. Positive attitudes toward handwashing stations followed a similar trend, with 86.7 percent of women agreeing that every house should have a handwashing station at baseline and increasing to 90.7 percent at endline. After the video screening, an important transition appeared to occur with regard to self-efficacy and self-reported/observed behaviors. At baseline, only 35.2 percent of women said they believed they could definitely have or install a handwashing station. This increased to 94.4 percent after the second survey and leveled off at 83.7 percent at endline. The increase in self-efficacy translated into higher levels of women stating that their household had at least one place designated to wash hands. At baseline, only 14 percent of all respondents had at least one place designated for handwashing. This increased to 48.8 percent after the second survey and reached 59 percent at endline.
Figure 4. Presence of a Handwashing Station: Knowledge, Attitudes, Self-Efficacy, and Behavior of Women with a Child Under Two Years by Survey Round
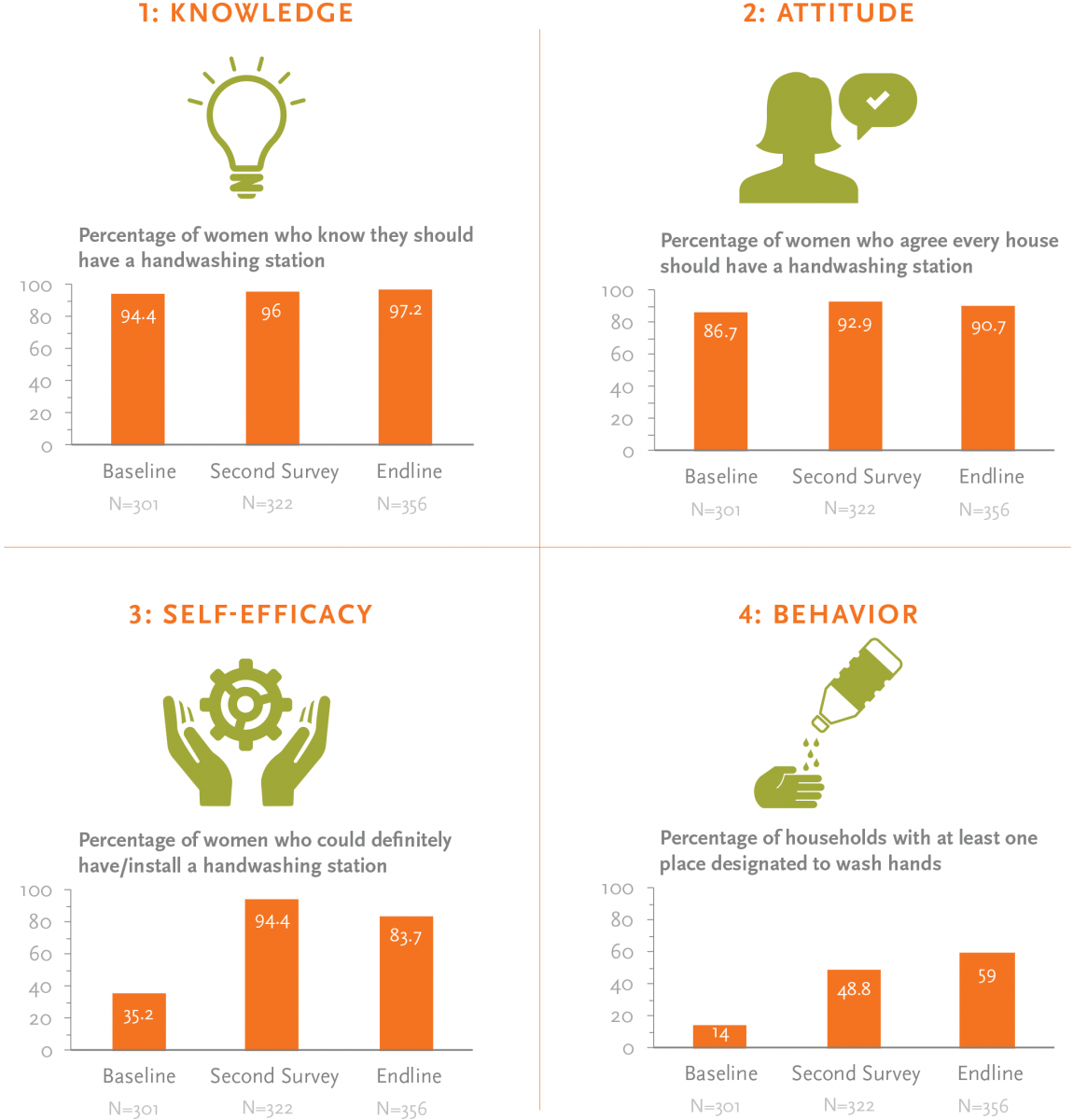
Figure 5. Percentage of Husbands and Women Responsible for Maintaining a Handwashing Station, According to Women with a Child under Two Years by Survey Round
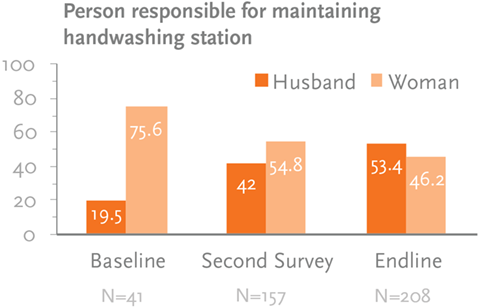
As discussed previously, men are often the decision makers in Niger households and enlisting their support is important for behavior change. As seen in Figure 5, at baseline, in the households with a handwashing station, only 19.5 percent of men maintained it. After video exposure, however, the percentage of men maintaining the handwashing station increased to 42 percent by the second survey and reached 53.4 percent at endline.
The video promoted the message that women should have a handwashing station near the kitchen and/ or latrine. Among women who had a handwashing station at baseline, the majority of the stations were located at the entrance of the compound (43.9 percent), followed by the kitchen, at 36.6 percent. At the second survey, however, 65.6 percent of women reported having a handwashing station next to the kitchen. At the endline, 52.9 percent of households had a handwashing station next to the kitchen and 44.2 percent of households had a handwashing station near the latrine, as recommended by the video. At baseline, of the 14 percent who had a handwashing station, 73.8 percent of women could present a handwashing station with soap and water during the interview. This increased to 95.5 percent at the second survey and reached 96.2 percent at the endline. (See Annex 1.)
Women were asked to cite critical times when it is necessary to wash hands. Before the meal was the most frequently cited time for washing hands (nearly 80 percent) at baseline. However, 4–8 weeks following the video, after using the latrine/defecation and before preparing a meal were the most frequently cited times for practicing handwashing behavior (81.4 percent and 86.6 percent, respectively). At endline, the higher levels of knowledge for critical times to practice handwashing persisted, as over 75 percent of women cited that they washed hands after using the latrine/defecation, after cleaning a child’s bottom, and before preparing a meal. When women were asked more specifically about the reasons they washed their hands, most women at baseline reported the reason to be preventing/ diarrhea/infection (83.7 percent). This increased to 93.5 percent following video exposure but dropped slightly 2–4 months after video exposure, to 85.1 percent. (See Annex 1.)
Overall knowledge of how to appropriately wash hands improved from baseline. At baseline, 88.1 percent of women were observed to wet hands with water, 78.6 percent applied soap, and 64.3 percent dried hands in the air rather than on a towel. Proper handwashing behaviors increased at the second survey and at endline. At endline, 92.4 percent of women wet hands with water, 95.7 percent applied soap, and 91.4 percent dried hands in the air rather than on a towel.
As shown in Figure 6, while over 90 percent of women at baseline agreed that you should wash your hands with clean water and soap, only 54.8 percent said they could definitely wash their hands with soap and clean water. Following exposure to the video, 97 percent of women said they agreed that you should wash hands with clean water and soap. This dropped slightly, to 94.4 percent, at endline. Women’s belief that they definitely could wash hands with soap and clean water increased to 98.4 at the second survey before declining to 90.4 percent at the endline. As with the handwashing station, after exposure to the video women showed an increase in self-efficacy that translated into improved handwashing behavior. At baseline, approximately 78 percent of women had a handwashing station with soap and water (among those with handwashing stations). This increased to 98.1 percent at the second survey and 95.7 percent at the endline.
Figure 6. Handwashing with Soap and Water, Knowledge, Attitudes, Self-Efficacy, and Behavior of Women with a Child under Two Years by Survey Round
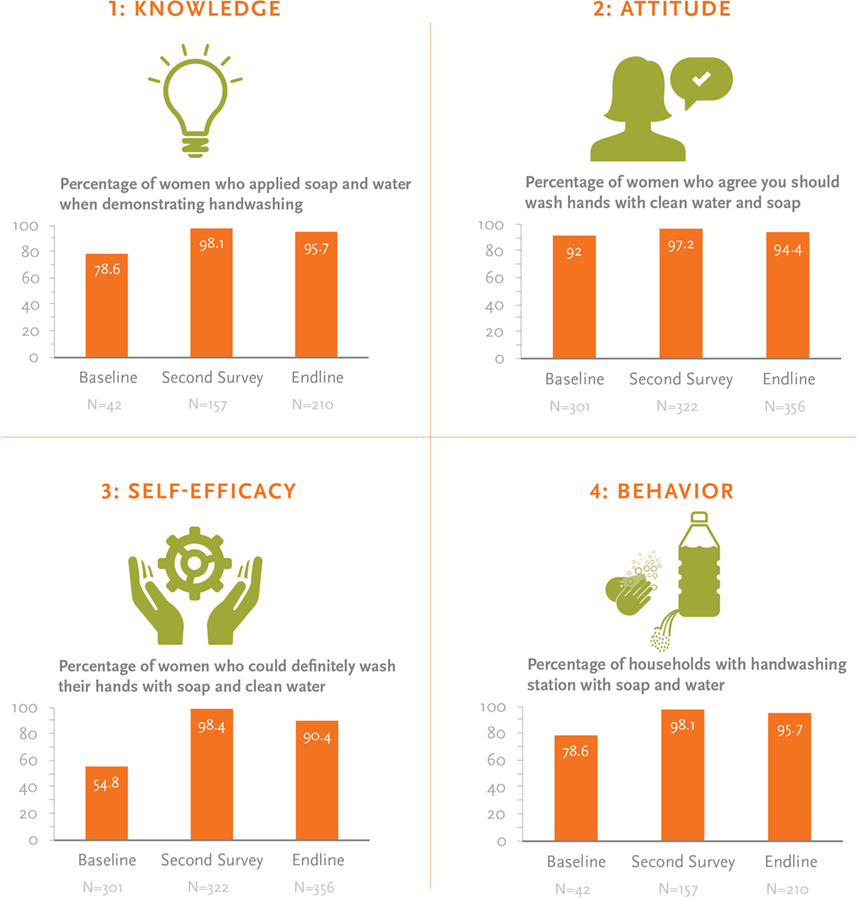
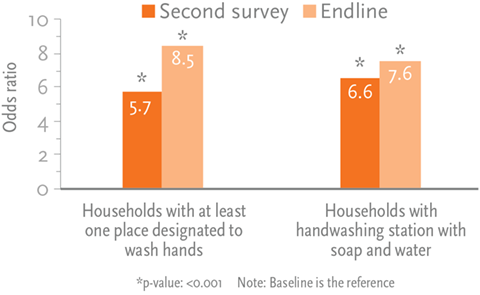
Figure 7. Logistic Regression Odds Ratios for Handwashing Behavior
To further assess the changes in behavior since exposure to the intervention, we ran logistic regressions on a subset of handwashing outcomes of interest while controlling for time and sociodemographics since exposure. Two independent variables were coded for time. The first time variable was for four to eight weeks following video exposure and the second time variable was for two to four months following video exposure. Sociodemographic control variables in the handwashing models included age of the woman, parity, and educational attainment.
The handwashing behavior models indicated that the odds were five to six times greater for women to have at least one place designated to wash hands and have a handwashing station with soap and water four to eight weeks following exposure to the video, compared to not having a handwashing station at baseline, while controlling for age, parity, and educational attainment. This effect increased at endline, where the odds were 8.5 times greater for women to have a designated place for handwashing and the odds were 7.6 times greater for women to have a handwashing station with soap and water when compared to the baseline. Figure 7 presents results from the handwashing behavior logistics regressions.
Responsive Feeding Behaviors
As shown in Figure 8, overall knowledge of responsive feeding behavior improved over time. At baseline, 46.5 percent of women said that they should provide encouragement to a child to eat.
Figure 8. Responsive Feeding, Knowledge, Attitudes, Self-Efficacy, and Behavior of Women with a Child under 2 Years by Survey Round
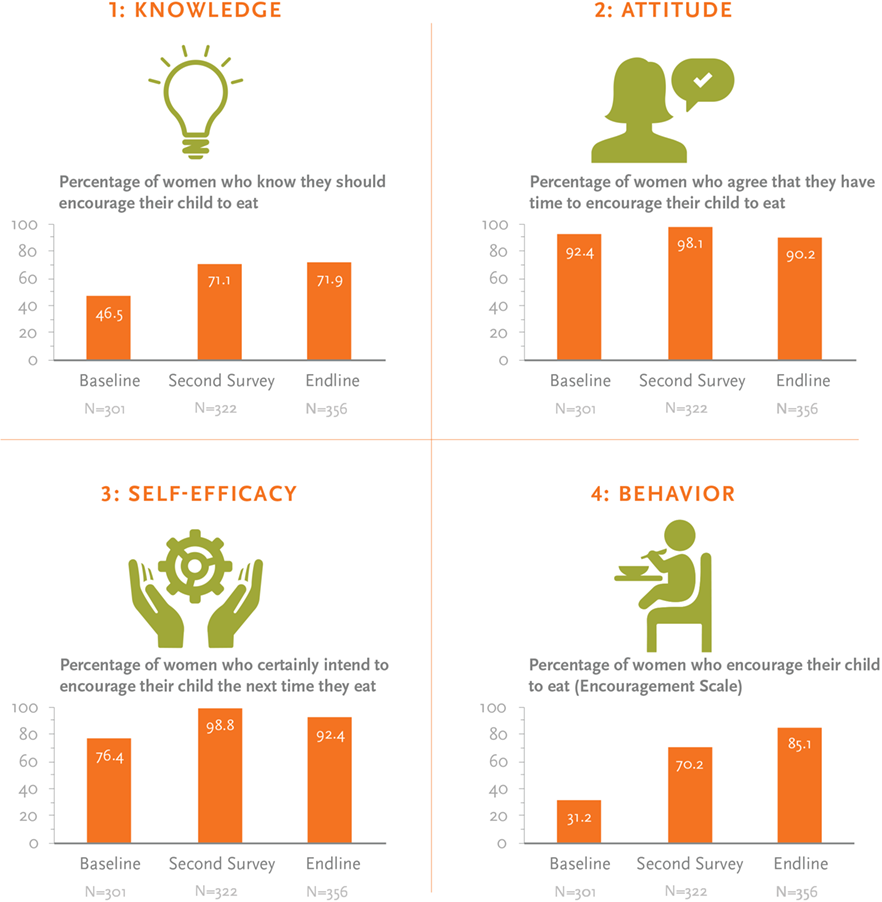
Following exposure to the video, the percentage of women saying that they knew they should provide encouragement to their child to eat increased to 71 percent. The percentage of women who agreed that they could sing and play to encourage their child to eat increased from 74.8 percent at baseline to 93.8 percent at endline, and the percentage of women who said they could encourage their child to eat increased from 76.4 percent at baseline to 92.4 percent at endline. At baseline, 31.2 percent of women actively encouraged their child to eat. This increased to 70.2 percent after video exposure and reached 96.6 percent at endline. The responsive feeding scale was calculated based on a battery of 20 validated questions that have been shown to measure if a caregiver is actively feeding the child.
As shown in Figure 9, we observed similar trends with the percentage of women who knew that a child should have a separate plate, which increased from 79.4 percent at baseline to 98.6 percent at endline.
Figure 9. Child Has a Separate Plate—Knowledge, Attitudes, Self-Efficacy, and Behavior of Women with a Child under 2 Years by Survey Round
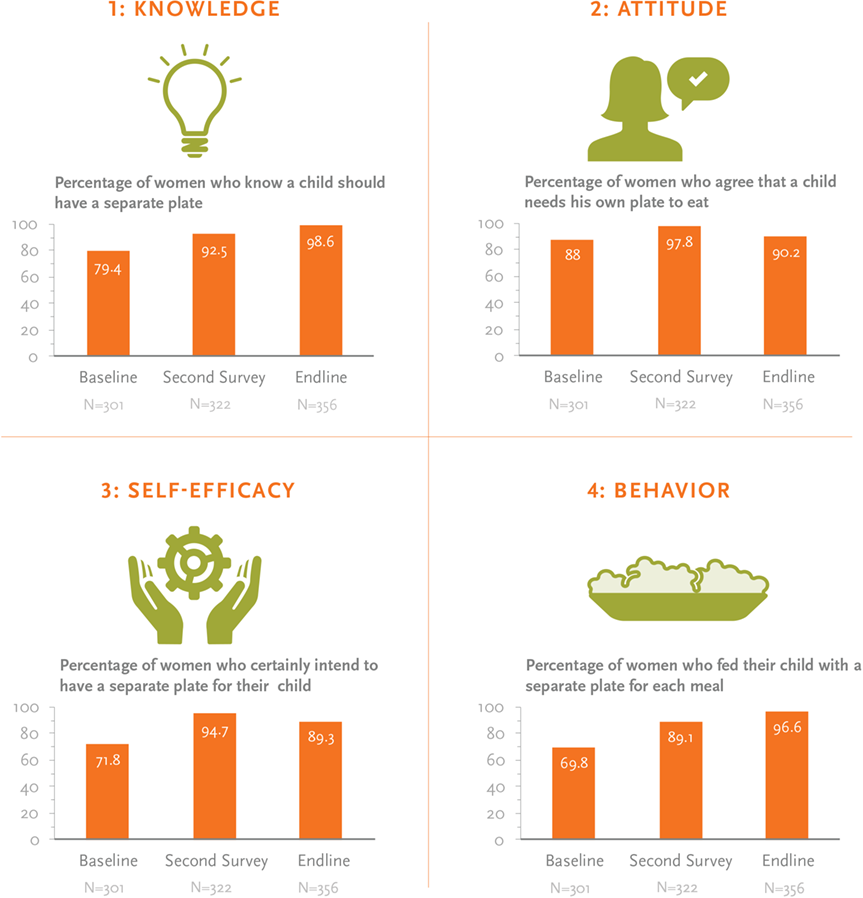
The percentage of women who agreed they could feed a child from a separate plate and encourage their child was slightly higher at the second survey than at endline. This may be because the endline survey data were collected during the peak farming season, when many women were busy in the fields. Among WRA who had a child in the two years preceding the survey, approximately 69.8 percent had a separate plate for their child at baseline. This increased to 89.1 percent at the second survey and reached 96.6 percent at endline.
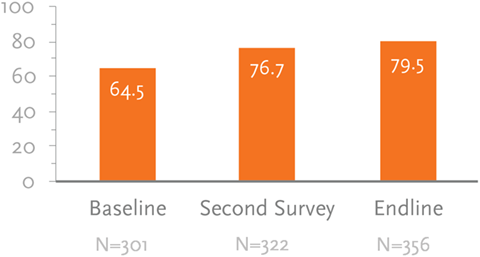
Figure 10. Percentage of Women Who Said That the Person Responsible for Helping the Child Was Less Than an Arm’s Length Away
The percentage of women who agreed a child should eat with a responsible person increased from 83.7 percent at baseline to 92.1 percent at endline, and a woman’s belief that she could ensure this behavior increased from 63.8 percent at baseline to 92.4 percent at endline. (See Annex 1.)
The percentage of women who agree that a child needs to be fed by a responsible person within arm’s length remained relatively the same across survey rounds. However, their belief that they could practice the behavior increased from 65.8 percent at baseline to 92.4 percent at endline. (See Annex 1.) Approximately two-thirds of women reported that a responsible person was less than an arm’s length away at baseline. As shown in Figure 10, this improved to 76.7 percent after video exposure and reached 79.5 percent at endline. We observed similar trends regarding a child receiving help from a responsible person at the last meal.
To assess the changes in behavior since exposure to the intervention, we also ran logistic regressions on a subset of responsive feeding outcomes of interest while controlling for time and sociodemographics since exposure. We coded two independent variables for time. The first time variable was for four to eight weeks following video exposure and the second time variable was for two to four months following video exposure. Sociodemographic control variables included age of the woman, parity, and educational attainment, as well as age and gender of the child.
Figure 11. Logistic Regression Odds Ratios for Responsive Feeding Behaviors
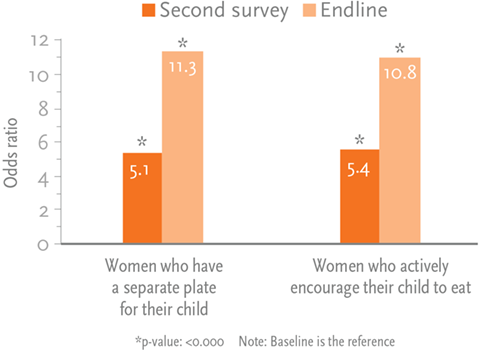
Results indicate that the odds were 5.4 times greater for women to actively encourage their child to eat at the last meal and the odds were 5.1 times greater to have a separate plate at 4–8 weeks when compared to baseline following exposure to the video while controlling for age, parity, educational attainment, and age and sex of the child. This effect increased at endline, when the odds were 10.8 times greater to actively encourage their child to eat at the last meal and the odds were 11.3 times greater to have a separate plate for the child when compared to baseline as shown in Figure 11.
Exposure to Handwashing and Responsive Feeding Messages
Overall, exposure to messages related to the two priority behaviors markedly increased following the baseline survey. As expected as shown in Figure 12 and Figure 13, video exposure was the most frequently cited source of messaging on both behaviors, which was 0 percent at baseline but increased to approximately 50 percent following introduction of the video sessions in the beneficiary groups. Exposure to messages from community meetings and volunteers increased after baseline and declined at endline, likely because the question was asked if the respondent had heard messages through these channels in the previous two weeks and the intervention had occurred a couple of months prior. With poor access to radio and television as well as low rates of literacy in the communities, it is not surprising that fewer than 5 percent of women cited posters, newspapers/magazines, government messages, radio or TV as a source of messaging. (See Annex 1.)
Figure 12. Source of Handwashing Message by Channel and Study Period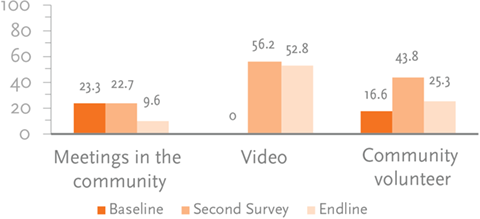 | Figure 13. Source of Responsive Feeding Message by Channel and Study Period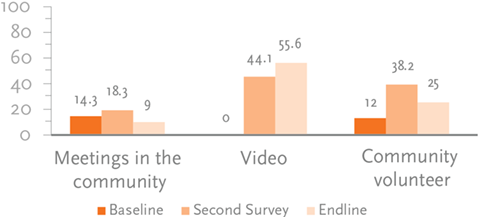 |
The evidence supports that the video screenings combined with home visits can lead to sustained behavior change. The survey found that the presence of a handwashing station increased from 14 percent at baseline to 48.8 percent at the second survey; this behavior was sustained and increased again at endline to 59 percent. We found a similar result with the responsive feeding indicators, where children who had a separate plate increased from 69.8 percent at baseline to 89.1 percent at the second survery; the behavior was sustained and increased to 96.6 percent at endline.
When asked who they shared messages with, the majority of women stated that they shared messages on handwashing and responsive feeding with their co-wives, husbands, friends, and neighbors as seen in Figure 14 and Figure 15. Of interest is the continued increase in women who share messages with family members, friends, and neighbors at endline, indicating that the intervention is continuing to diffuse throughout the community.
Figure 14. Percentage of Women Who Shared Handwashing Message by Person and Survey Round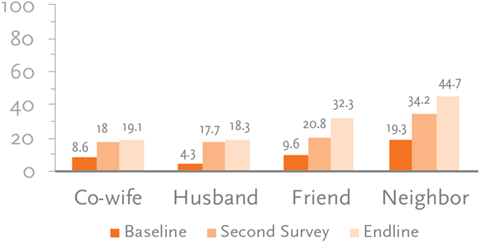 | Figure 15. Percentage of Women Who Shared Responsive Feeding Message by Person and Survey Round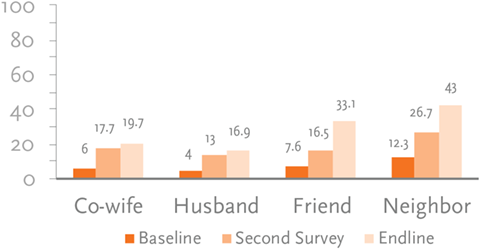 |
Cost and Scale-Up
The section that follows presents results from the cost analysis. We discuss the cost per person reached and behavior changed as well as present the costs associated with scaling up the pilot intervention to new communities and introducing new videos. We also include factors to consider when scaling up the pilot intervention.
Cost Analysis
Our detailed analysis of the intervention expenditures determined that the total cost for the current intervention in the selected villages was US$242,804. The costs included various trainings, the video production work, the monthly meetings with community mediators, monitoring and supervision both remotely and through field trips, the establishment of the information and monitoring system to ensure quality, the dissemination of the community videos, and follow-up visits to group members by the community mediators. Additional details on the cost per program component are available by request in the full cost analysis report (Minault 2015). Based on information collected through routine monitoring, the proof of concept estimates that 1,500 individuals in the 20 communities were reached through the intervention. Results of the cost per beneficiary and behavior change by various cost scenarios are presented in Table 3.
Table 3. Cost per Beneficiary and for Scaling Up the Intervention
| Proof of Concept | Scenario 1 | Scenario 2 | ||||
|---|---|---|---|---|---|---|
| N | US$242,804 | N | US$277,169 | N | US$304,887 | |
| Cost per person reached | 1,500 | $16.19 | 7,500 | $3.73 | 7,500 | $4.13 |
| Number of households at endline that have one place designated to wash hands | 840 | $28.91 | 4,200 | $6.60 | 4,200 | $7.26 |
| Number of households at endline with handwashing station with soap and water | 501 | $48.46 | 2,505 | $11.06 | 2,505 | $12.17 |
| Number of new women who have a separate plate for their child at endline | 670 | $36.24 | 3,350 | $8.27 | 3,350 | $9.10 |
| Number of new women who actively encourage their child to eat | 624 | $38.91 | 3,120 | $8.88 | 3,120 | $9.77 |
Based on these estimates, we were able to derive a cost per beneficiary reached, which was approximately US$16.19 per person. This estimate was derived by taking the total cost of the proof of concept phase and dividing by the 1,500 beneficiaries and the 10 behavior change messages to which the individuals were exposed. We then examined the difference in the baseline and endline values for two key behaviors that the proof of concept aimed to change. For the handwashing behavior, we extrapolated that 840 of the 1,500 beneficiaries had changed behaviors, based on the change from a baseline of 14 percent to an endline value of 59 percent. We used a similar extrapolation method to determine the number of beneficiaries who adopted the separate plate behavior change, and arrived at 670 beneficiaries.
Based on the number of beneficiaries whose behaviors changed, we determined the cost per handwashing behavior changed to be US$28.91 per beneficiary and US$36.24 per beneficiary who adopted the separate plate behavior. It is important to note, however, that the above costs reflect a small proof of concept phase, which tends to be more expensive as a result of scoping and start-up costs and does not benefit from economies of scale.
Potential for Scale-Up
Enthusiasm for the videos has extended beyond the immediate communities, and we have noted interest in expanding the video disseminations to new audiences, considering new means of projecting the videos, and increasing the number of mediators.
We must extend the video sessions for all other groups of villages and go to neighboring villages. By increasing the number of mediators and finding alternative means of projection, including CD recordings and cell phones, we can expand the program reach.
—Male mediator
We estimated the scale-up costs for two scenarios. Scenario 1 included scaling up the intervention to an additional 100 villages (i.e., 7,500 beneficiaries) in the region of Maradi using the existing 10 videos produced by the proof of concept. To scale up the program, costs were estimated to increase to US$277,169. The primary drivers of the increased cost are labor and activity; using existing videos will result in some cost savings. As a result, the cost per beneficiary drops to US$3.73 per person reached, US$6.60 for the handwashing station behaviors changed, and US$8.27 for the separate plate behavior.
A second cost scenario included scaling up to 100 villages in a new region in the Sahel, which would require additional formative research, training tool adaptation, and production of new video content. The costs associated with the second scenario were US$304,887. As a result, the cost per beneficiary would be US$4.13 per person reached, US$7.26 for the handwashing station behaviors changed, and US$9.10 for the separate plate behavior.
Results from the FGDs identified factors that should be considered for future scale-up activities.
Future Training Needs for Mediators
The introduction of video screening to existing group meetings could benefit from additional external support. Several mediators commented that the monthly refresher trainings were important to reinforce their understanding, introduce new content, and obtain responses to unanswered questions.
Some mediators, however, felt that even without continued external support, if the equipment and videos were made available to them, they could continue with the home visits to counsel the populations and expand the reach of the pilot intervention.
If the project does not remove the equipment, we could continue to provide home visits and advise the population.
—Mediator
Ideas for Future Video Topics
Beneficiaries provided feedback on topics for new videos that they would be interested in seeing if the pilot intervention was extended. Some suggestions included videos on contraceptive methods and birth spacing; the importance of education, particularly among young girls, and avoiding early marriage; adolescent nutrition; water treatment; and advice on methods for improving agricultural practices.
Mediators and beneficiaries made several additional suggestions that may be useful to address if activities are scaled up in the future. Beneficiaries and mediators felt it would be helpful to show the risks of not adopting the behaviors in the videos, to provide videos with subtitles, or to provide written brochures and/or visual aids that could be shared with household members and to provide a summary of the key issues at the conclusion of the video. Several other suggestions included using SMS messages to remind beneficiaries of the subjects promoted, and to provide T-shirts or rewards to beneficiaries who changed behaviors.
Discussion and Conclusion
The community video approach used in this study proved effective in influencing knowledge, attitudes, self-efficacy, and self-reported behaviors in the resilience setting of Niger.
Findings from the mixed-methods evaluation suggest that our community video approach is an acceptable and effective tool to support MIYCN behavior change in the resilience setting of Niger. Below, we present a summary of research findings as well as recommendations to inform future efforts.
Exposure to messages through multiple communication channels supports diffusion of information.
Findings from both the quantitative and qualitative data suggest that the multiple communication channels introduced through the pilot intervention are effective at generating discussion within communities, which may in turn may influence social norms and make the messages of community video more sustainable. According to the quantitative surveys, exposure to handwashing and responsive feeding messaging through the video channel increased from 0 percent at baseline to over 50 percent at endline. Similarly, exposure to messages from community volunteers through home visits increased from approximately 15 percent for both behaviors at baseline to approximately 40 percent at endline. The increases in exposure to information through videos and home visits coincided with an increase in the number of women who exchanged information regarding both handwashing and responsive feeding behaviors with a number of community members, including the village chief, friends, and neighbors. Findings from the qualitative interviews suggest that beneficiaries would like to receive continued support through home visits after each video screening. Specifically, the women mentioned the need to reinforce the messages shared through the videos screenings, the importance of sharing the information with other members of the household, and the need for support with behavior adoption.
We recommend that future activities consider studying the levels of exposure needed to support diffusion of information as well as how the spread of information influences behavior change. This information can help determine the optimal “dose” of exposure to video exposure and home visits needed to achieve behavior change.
Inviting influencers, especially husbands, to pilot intervention activities increases their support.
The importance of men’s role in supporting behavior change emerged in both the qualitative and quantitative findings. Survey data indicate the increasing involvement of men in supporting handwashing behavior; the percentage of men maintaining the handwashing station increased markedly, from 19.5 percent at baseline to 53.4 percent at endline. The percentage of women who said that they had discussed the handwashing and responsive feeding health messages with their husbands also increased. Findings from the qualitative interviews supported this evidence, showing that men were providing support for women by installing handwashing stations, allowing women to go to the health facility, and ensuring that their children were being fed.
Since male decision making serves as a major determinant influencing a woman’s ability to adopt a healthy behavior, future research may seek to gather data on changes in the knowledge, attitudes, and practices of men and draw comparisons across women and men, looking at where their knowledge, attitudes, and practices are concordant and discordant. Understanding differences in how men and women respond to behavior messages would help identify where more targeted communications can be developed to address differences.
There is enthusiasm for scaling up the pilot intervention and costs will decline per beneficiary.
Findings from the qualitative interviews suggest that enthusiasm for the videos has extended beyond the immediate communities and new audiences in surrounding communities are interested in viewing the videos. Pilot communities are also interested in new video themes. Results from the cost analysis indicate that costs will drop considerably as the pilot interventions are taken to scale. The cost associated with expanding the intervention from 1,500 to 7,500 beneficiaries and introducing new video content was estimated to be US$304, 887. As a result, the cost per beneficiary would be US$4.13 per person reached, US$7.26 for the handwashing station behaviors changed, and US$9.10 for the separate plate behavior. Although we cannot compare cost estimates from previous studies because different investigators used different assumptions, we can place the price per behavior change in context with similar interventions. When considering costs of similar interventions, studies have looked at the cost per life saved and found that costs ranged from US$22 per year of life saved to as high as US$393 (Farnsworth et al. 2014).
It is important to note that we introduced the pilot intervention in an area where partners had an established presence. This means that costs do not reflect the effort that partners have invested to engage communities, develop rapport with community leaders, and achieve their support for activities. In addition, previous studies have noted that community-based intervention should assess and address communities at the various stages of community readiness for change, recognizing that not all communities are ready to receive information and take steps toward change. Future efforts should take into account stages of community readiness and tailor interventions to meet communities at their stage of readiness for behavior change. Future efforts should also more actively engage with the government health system to explore how the approach can be integrated into or adopted by existing health worker platforms.
The SPRING/DG collaboration in Niger shows that the approach can be implemented successfully in the resilience context of Niger. Results from our mixed-methods evaluation highlight the potential of the community video approach as an innovative and effective approach for fostering both social and individual nutrition and hygiene-related behavior change. Overall, results show that using multiple channels for disseminating messages and engaging with key influencers is a promising approach to empower women, men, and communities to improve their health through improved nutrition and hygiene behaviors.
Footnotes
1 Defined as falling below –2 standard deviations from the median height-forage of the WHO reference population.
2 The four existing groups included men’s groups (model husbands selected by health center, 25–60 or more years), adolescent girls’ groups (12–18 years), and several types of groups with women of reproductive age (15–49 years). Each group contained approximately 10–25 participants who benefited from the monthly video screening, facilitated discussion, and home visit.
3 A tippy tap is a hands-free way to wash hands in rural settings where there is no running water. The tippy tap includes a small cup or gourd that contains water. The cup is tipped to allow running water to flow for handwashing.
References
Bandura, A. 2004. “Health Promotion by Social Cognitive Means.” Health Education & Behavior 31(2): 143–64. http://doi.org/10.1177/1090198104263660
Bentley, M. E., H. M. Wasser, and H. M. Creed- Kanashiro. 2011. “Responsive Feeding and Child Undernutrition in Low- and Middle-Income Countries. ” Journal of Nutrition 141(3): 502–507. http:// doi.org/10.3945/jn.110.130005
Berrigan, F. 1979. Role of Community Media in Development. Paris: United Nations Educational, Scientific and Cultural Organization.
Black, R. E., L. H. Allen, Z. A. Bhutta, et al. 2008. “Maternal and Child Undernutrition: Global and Regional Exposures and Health Consequences. ” Lancet, 371(9608): 243–60.
Desta, B. F., H. Mohammed, D. Barry, A. H. Frew, et al. 2014. “Use of Mobile Video Show for Community Behavior Change on Maternal and Newborn Health in Rural Ethiopia.” Journal of Midwifery & Women’s Health 59(s1): S65–S72. http://doi. org/10.1111/jmwh.12111
Farnsworth, S. K., K. Böse, O. Fajobi, P. P. Souza, et al. 2014. “Community Engagement to Enhance Child Survival and Early Development in Low- and Middle-Income Countries: An Evidence Review.” Journal of Health Communication 19(1): 67–88. http://doi.org/10.1080/10810730.2014.941519
Institut National de la Statistique (INS)and ICF International. 2012. Enquête Démographique et de Santé et à Indicateurs Multiples du Niger 2012 [French]. [Multiple Indicator Demographic and Health Survey.] Calverton, MD: INS/ICF International.
Kadiyala, S., T. Roopnaraine, A. Margolies, and S. Cyriac. 2014. Using a Community-Led Video Approach to Promote Maternal, Infant, and Young Child Nutrition in Odisha, India: Results from a Pilot and Feasibility Study. Arlington, VA: Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project.
Khoury, A. J., A. K. Mitra, A. Hinton, et al. 2002. “An Innovative Video Succeeds in Addressing Barriers to Breastfeeding among Low-Income Women.” Journal of Human Lactation 18(2): 125–31.
Minault, S. 2015. SPRING/Digital Green: Analyse des coûts [French]. [SPRING/Digital Green: Cost Analysis.] Arlington, VA: Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project.
Moreaux, M. 2015. Informing Video Topics and Content on MIYCN and Handwashing: Situational Analysis and Formative Research in Maradi, Niger. Arlington, VA: Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project.
Roye, C., and M. Hudson. 2003. “Developing a Culturally Appropriate Video to Promote Dual-Method Use by Urban Teens: Rationale and Methodology.” AIDS Education and Prevention 15(2): 148–58.
Stokols, D. 1996. “Translating Social Ecological Theory into Guidelines for Community Health Promotion.” American Journal of Health Promotion 10(4): 282–98.
Tuong, W., E.R. Larsen, and A. W. Armstrong. 2014. “Videos to Influence: A Systematic Review of Effectiveness of Video-Based Education in Modifying Health Behaviors.” Journal of Behavioral Medicine 37(2): 218–33. http://doi.org/10.1007/ s10865-012-9480-7






