
SPRING, a six-year project (2012 to 2017), is supported by the United States Agency for International Development (USAID). Established in April 2012, SPRING/Uganda’s primary goal is to contribute to the reduction of stunting in children between 0–23 months of age, anemia in children 0–23 months of age, and women of childbearing age. We provide technical assistance and leadership at the national level to implement activities and policies related to large-scale food fortification—via industrial fortification and micronutrient powders—to address stunting and micronutrient deficiencies, prevention and control of anemia through multi-sectoral coordination, and social and behavior change communication (SBCC) for nutrition.
In addition to supporting national-level activities, SPRING delivered nutrition services to improve the nutritional status of mothers and children in the Southwest (SW) and East Central Regions of Uganda. USAID asked SPRING to support the reestablishment of the nutrition assessment, counseling, and support (NACS) continuum of care in nine former NuLife-supported hospitals; and expand NACS services to 35 health centers in the districts of Kisoro and Ntungamo in the SW region. NACS, a client-centered platform, ensures service integration along the continuum of care within the context of HIV/AIDS, maternal and child health, and the health system. Our NACS interventions strengthened the capacity of facility- and community-based health care providers to deliver nutrition-specific services while linking clients to nutrition-sensitive interventions provided by the health, agriculture, food security, social protection, education, and rural development sectors.
By May of 2015, when this initiative ended, SPRING/Uganda had provided technical assistance to district health offices and health centers in Kisoro, Namutumba, and Ntungamo to integrate NACS in 51 facilities, across 12 districts. We also provided technical assistance to the U.S. Centers for Disease Control and Prevention-funded Makerere University Joint AIDS Program (MJAP) to integrate NACS into its 10 supported health centers in Mbarara District, and to HealthPartners Uganda for NACS integration at health centers in Ibanda, Mbarara, and Bushenyi Districts.
This brief describes SPRING’s challenges and achievements using the NACS approach in Uganda to integrate nutrition into the health care delivery system.
Objectives
The purpose of the endline assessment is to assess the status of NACS programming, appropriateness, relevance, effectiveness, and sustainability of interventions in supported health facilities, and to document key lessons learned and best practices.
The assessment sought to—
- Examine the effectiveness of the SPRING/Uganda programming to improve NACS integration within the established timeframe.
- Measure all the outcomes of SPRING’s interventions on health facilities and beneficiaries.
- Assess the acceptability and adoptability of the approach from the standpoint of the health facility staff.
- Within the existing health structures, examine the feasibility of integrating NACS.
- Determine the principle factors that motivate or inhibit health workers and village health teams (VHTs) to provide NACS services at the facility and community level.
- Assess the role of community health workers in delivering preventive and/or curative nutrition services to vulnerable groups, including people living with HIV (PLWHIV).
The assessment also compared endline results to previous similar surveys to measure the extent to which facility performance may have improved over time. Because the assessment took place almost a year after SPRING’s NACS interventions and support to the health facilities had ended, it was an opportunity to investigate whether improvements were sustained.
Design and Approach
SPRING used a cross-sectional design for this assessment, which included a mix of qualitative and quantitative methods to assess the effectiveness of the NACS interventions. Past reports and formative assessments were reviewed and triangulated with a baseline study that SPRING conducted in 2013. We collected health facility data and reviewed client records for the quantitative analysis; key informant interviews and focus group discussions with beneficiaries and VHTs were the basis for the qualitative information collected. For this assessment, we adapted 12 sets of data collection tools from prior SPRING studies.
Key Findings
A total of 50 health facilities in 10 districts were included in this assessment. SPRING reached 63 respondents through key informant interviews (KIIs) and 132 people participated in focus group discussions. The majority (84 percent) of the health facilities were government owned. SPRING’s performance monitoring plan included 57 indicators and 2 sub-intermediate results.
Training and Human Resources for Health Capacity Development
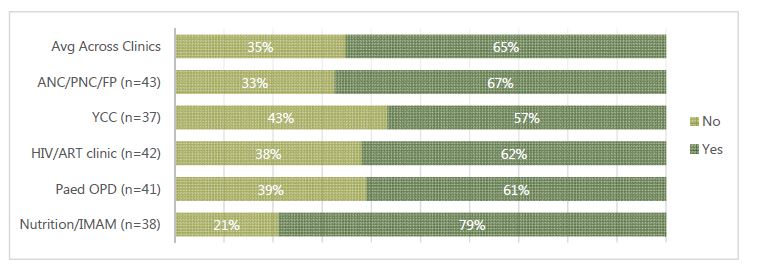
Building institutional capacity was an integral component of the NACS programming. On-the-job training, mentorship, support supervision, and related capacity enhancement aspects of human resources for health were included in the implementation. The majority (65 percent) of staff trained by the project were still in service at the time of the endline assessment. Figure 1 summarizes the percentage of health workers trained in NACS; it shows that the nutrition unit and the antenatal care (ANC)/maternity units had the most participants in the trainings.
Figure 1: Percentage of Health Facility Staff Trained in the NACS at Endline
In addition to training health facility staff, NACS programming advocated for nutrition-specific positions and a multi-sectoral approach to be included at the district and health facility level; the next cycle of programming should continue to push for both levels to include these components.
Availability of Nutrition Guidelines and Protocols
On average, 26 percent of the service delivery points in the surveyed health facilities had the different nutrition-specific guidelines and protocols available. From table 1, Nutrition/Integrated Management of Acute Malnutrition (IMAM) (36 percent) and HIV/antiretroviral therapy (ART) (34 percent) clinics had the highest protocol and guidelines availability, which shows the SPRING/NACS focus on the most vulnerable groups, specifically HIV+ mothers and the exposed infants. On the other hand, within the pediatric Outpatient Department (OPD) clinics at the health facilities, nutrition-specific guidelines and protocols were not as common (12 percent). In addition, while availability of the guidelines was relatively high, their use remained extremely low. Only 17 percent of the facilities reported using the Baby-Friendly Hospital Initiative guidelines, while 15 percent and 34 percent reported using the infant and young child feeding policy and IMAM guidelines, respectively.
Table 1: Availability of Nutrition Assessment Guidelines/Protocols at Service Delivery Points
| Number of Service Delivery Points With Protocols or Guideline for Nutrition Assessment | ANC Maternity PNC /FP | YCC | HIV/ART Clinic | Pediatric OPD | Nutrition/ IMAM | Percentage |
|---|---|---|---|---|---|---|
| Not available | 41 | 40 | 30 | 44 | 32 | 74% |
| Available | 9 | 9 | 17 | 6 | 18 | 26% |
“We have applied the mentorship model to scale up and strengthen NACS implementation at all levels and it has shown improvement... The approach followed is the structures of government are the ones we use to implement nutrition activities. In this nutrition is implemented at the district level, health facilities, sub-county and the community level.” KII_Nutrition focal person
“We have what we call the district nutrition coordination policy since nutrition problems do not rise only from the health department and cannot be managed by only health department. So it’s a requirement by the ministry of health for all districts to have a health coordination committee comprising of different district departments (water, agriculture, community, health, administrative to oversee and plan for nutrition activities, and we regularly update our political side because they are the mobilizers of the communities” KII_Namutumba focal person
Ownership, Service Integration, and Sustainability
SPRING’s NACS implementation approach focused on activities that align with the UNAP 2012–2016— supporting the existing structures of the local government and communities for the sustainability of services. This advocated for district local government structures to consider nutrition as an integral component to attain the Uganda Minimum Health Care Package. The revitalization of the District Nutrition Coordination Committees (DNCC) and Sub-County Nutrition Coordination Committees (SNCC), district leader commitment, and integration of nutrition activities into district work plans all point to the shared commitment, participation, and coordination of efforts toward the sustainability of nutrition services.
Nutrition Assessment
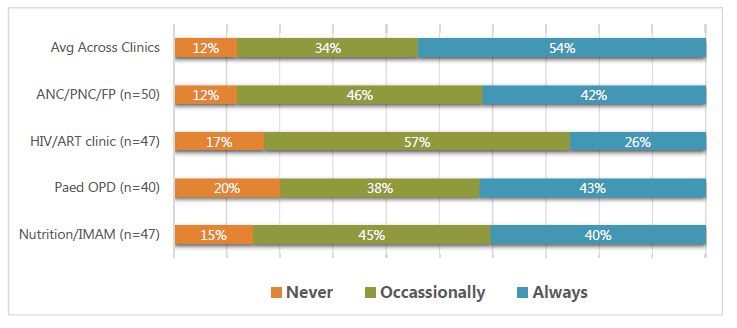
On average, up to 14 percent (see figure 2) of all units in the health facilities never carry out any type of nutrition assessment; however, 54 percent of the facilities were implementing consistent nutrition assessment practices. The nutrition assessment included measuring weight, irrespective of the age and situation of the patient; optimal referral within the health facility for key health services required by both the patient and attendant (e.g., HIV counseling services, sexually transmitted disease treatment, and immunization services); and providing vitamin A and any other required supplement (if available), at the appropriate time. Health workers cited workload and other institutional challenges as possible reasons for the failure of consistent nutrition assessment practices. In addition, the availability of equipment to conduct assessments also improved from 30 to 80 percent for length/height boards, and 90.5 percent of all weighing scales at the health facilities were in working condition.
Figure 2: Consistency of Carrying Out Nutrition Assessment across Facilities and Clinics
Nutrition Counseling
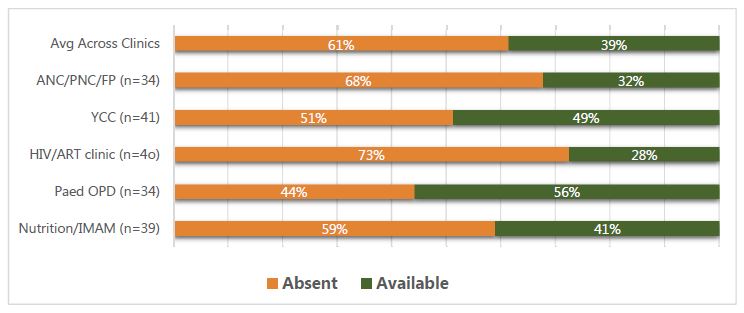
SPRING assessed the nutrition counseling by examining the availability of the required tools, clientele served, and arrangements for effective nutrition counseling. Tools and guidelines for nutrition counseling were only available at an average of 39 percent of clinics assessed (see figure 3). Nutrition counseling tools were least available at the HIV/ART clinics (28 percent) and most common at the pediatric OPD clinics (56 percent), followed by the Young Child Clinic (YCC) (49 percent). Levels of utilization of those tools remain low outside the nutrition/IMAM units of the health facilities.
Figure 3: Availability of Tools/Guidelines for Nutrition Counseling by Type of Clinic
On average, 57 percent of clinics reported providing nutrition counseling at every visit, which is an improvement. However, while an average 54 percent of clinics provided space for documenting nutrition counseling, only 60 percent of these facilities used that space regularly.
Nutrition Support
SPRING’s assessment of nutrition support analyzed the services provided to the targeted population. We had a limited role in controlling the supply of nutrition supplements/medicines and other products. However, the NACS—a component of SPRING—helped increase demand for these supplies that, in turn, contributed to their increased availability at health facilities.
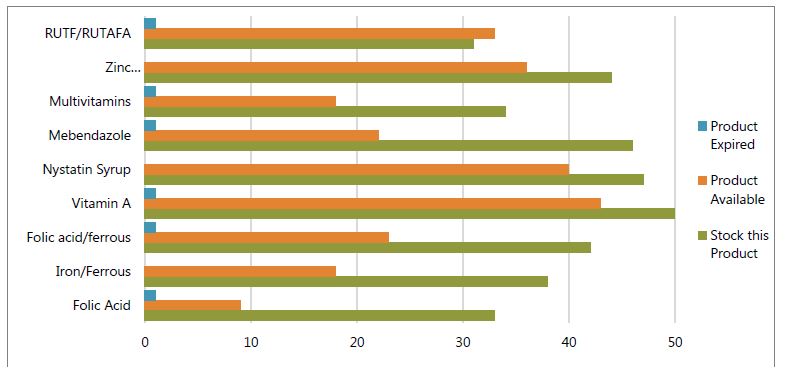
The assessment found that NACS programming improved the availability of essential nutritional supplies because facilities were more likely to order products, especially with the existing capacity support from other partners in the supply chain sector. Between 2013 and 2015, stockouts declined from an average of 17 percent to 7 percent. The majority (81 percent) of facilities reported stocking all the essential nutrition supplies; 54 percent had them on the day of the team’s visit, although 12 percent had expired products in stock (see figure 4). The essential nutrition supplies had the longest stockout, averaging 52 days, followed by other nutrition supplies at 39 days. The nutriceuticals averaged 30 days of stockouts in a year. There was an extremely long stockout for iron–folic acid and folic acid, at 63 and 90 days, respectively.
Figure 4: Stocking and Availability on Day of Visit and Reported Expiry of Essential Nutrition Supplies (n=50)
Referrals between the community and the facility are an important part of support. Clients should be referred from the VHT to the clinic, to the health center, and to the hospital as the severity of their condition requires. Similarly, clinics and hospitals should refer clients back to VHTs for more local and continued support. No evidence was found of referrals for clients from health facilities to VHTs and to community economic strengthening, livelihoods, and food security services; we found limited documentation of referrals within the health facilities. However, in-depth interviews with the beneficiaries indicated that the VHTs followed patients to the health centers, and back into the communities, to ensure they improved. In addition, VHTs reported they were trained and participated in the health facility outreach activities, and they followed up with patients from the communities to the health facilities.
Participation of VHTs in Provision of Nutrition Services
"Community volunteers advise us to eat foods that will build our bodies and fruits because food itself has roles it plays within the body...Things such as nakati, dodo, fruits they encourage us to eat." -Beneficiary testimony
The community component of NACS focused on mobilization, community-led assessment, effective referrals, and follow up with vulnerable groups, including PLWHIV. VHTs played a key role in bringing NACS work to the community level. Trained in this work, they played a role in all phases—from community mobilization, to health education, continued counseling and support, and the provision of referrals.
VHT fatigue was evident. While some VHTs may have been motivated by the additional requirements asked of them, and the training received, for others, this was a burden. Measures should be considered to alleviate any additional strain felt by the VHTs because of NACS.
Key Emerging Themes and Issues
A number of key issues need attention and/or strategic direction in the next project like this one. Such issues include—
NACS is a positive model of services integration
Despite the challenges and resistance faced at different stages of implementation, NACS remains a model for integrated service delivery. With improved programming and adaptability to context, scaling up NACS could improve nutrition outcomes at the facility level.
Integration of NACS approach within routine health services is possible
It is possible to integrate NACS within the routine health services if a systems approach is used to address issues of in-house capacity building, policy strengthening, health management information system (HMIS) review, and overall supply management.
Possibility of a community system-led nutrition program
Few VHTs were trained in NACS, yet their strong involvement and drive suggest promising possibilities for designing and implementing community-led nutrition programs. The quality of nutrition-related documentation needs to improve.
Non-facility–based capacity building is not sustainable
Classroom training was not sustainable and it did not necessarily contribute to long-term staff capacity building. In the future, capacity building should focus on facility-based mentorship programs to improve knowledge transfer/retention.
Availability of essential supplies and tools key to attaining results
The limited availability and range of essential nutrition supplies affected outcomes in certain areas. The current program at the national level pays less attention to nutrition supplies than other essential medicines and health supplies.
Multi-sectoral policy and coordination is essential for success
Coordination with other sectors is important for nutritional support to be successful. A multi-sectoral approach will promote a referral to social services that address food security and livelihood, improves the supply of required essential nutrition supplies, and strengthens community advocacy.
Conclusion and Way Forward
Overall, implementation was generally satisfactory. A number of key milestones and results were achieved by the end of the last quarter of 2015. This study found that project outputs and outcomes have been sustained across districts and health facilities one year after SPRING programming concluded in Uganda.
Some specific recommendations for consideration include—
- Providing stronger advocacy for nutrition policies and practices to create an enabling environment that supports NACS integration in the health system of Uganda. District-led programming will improve sustainability and ownership.
- Engaging the Ministry of Health is critical to strengthening the integration, filing, and reporting of nutrition parameters using the current HMIS and ART tools and reporting forms. A functional nutrition working group is required.
- Using data for continuous quality improvement at the district and health facility levels is absolutely necessary.
- Including the community-led nutrition counseling and support as a key component for improving malnutrition in the current draft community health extension workers (CHEWs) strategy, which the Ministry of Health is currently developing.
- Integrating the nutrition supplies into the routine health supply system to improve availability, readiness, and utilization of nutrition.
