October 2014–March 2015
Community‐based infant and young child feeding (IYCF) promotion, counseling, and support has been acknowledged as one of the key pillars of IYCF strategies in many countries. In 2009, the United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO) agreed that a global generic IYCF training package for community health workers was needed to complement the existing WHO/UNICEF Breastfeeding, Complementary Feeding and Infant and Young Child Feeding Integrated Counselling training package. It was specifically designed for facility health workers.
In response, UNICEF developed the Community Infant and Young Child Feeding (C‐IYCF) Counselling Package. The package was finalized and field tested under a strategic collaboration between UNICEF/New York and the combined technical and graphics team of Nutrition Policy and Practice (NPP) and the Center for Human Services—the not‐for‐profit affiliate of University Research Co., LLC (URC/CHS). The first edition of the C‐IYCF Counselling Package was published at the end of 2010 and was updated in 2012 and 2013.
The C‐IYCF Counselling Package is a resource designed to equip community volunteers (CVs) and primary health care staff to support mothers, fathers, and other caregivers to optimally feed their infants and young children. The training component of the package prepares CVs with technical knowledge on the recommended breastfeeding and complementary feeding practices for children from 0–24 months old and the optimal nutrition practices for pregnant and lactating women. In addition, the training enhances their practical skills in group facilitation, interpersonal communication and counseling, support to mothers and caregivers, problem solving, and reaching‐an‐agreement (negotiation) skills; and it prepares them to effectively use the related counseling tools and job aids.
The various elements of the C‐IYCF Counselling Package are based on WHO/UNICEF IYCF guidance documents, training, and other materials; including the WHO/UNICEF Breastfeeding, Complementary Feeding and Infant and Young Child Feeding Integrated Counselling training courses. The package also builds on materials developed by the Academy for Educational Development’s LINKAGES Project; the CARE USA and URC/CHS collaboration in Dadaab, Kenya; and the Integration of IYCF Support into Community Management of Acute Malnutrition (CMAM), produced by the ENN/IFE Core Group and IASC Global Nutrition Cluster. The technical content of the package aims to reflect the Guidelines on HIV and Infant Feeding 2010: Principles and Recommendations for Infant Feeding in the Context of HIV and a Summary of Evidence, which is related to IYCF in the context of HIV.
The package includes specific guidance for adapting it at the country level, especially aspects related to developing messages that target cultural barriers to optimal breastfeeding and complementary feeding practices. Included are the guidance and tools for data collection, monitoring, quality assurance and supervision, as well as the development of contextually appropriate local graphics for training aids and counseling material—essential elements intended to ensure an effective, sustained, and quality program. To date, approximately 30 countries are at various stages of adapting the C‐IYCF Counselling Package to the local context, building capacity, and rolling out community‐based IYCF programming.
Rationale and Objectives

Despite the global interest in the C‐IYCF Counselling Package, very little is known about its impact on IYCF behaviors in the countries where it has been adapted. For this reason, high‐quality studies are needed. Nigeria offers a unique opportunity to address this major gap in global evidence because the Federal Ministry of Health (FMOH), with support from two USAID‐funded global nutrition projects—the Infant and Young Child Nutrition Project (IYCN) and the Strengthening Partnerships, Results, and Innovations in Nutrition Globally project (SPRING)—has made a significant investment in adapting the generic C‐IYCF Counselling Package to the Nigerian context, including its translation into six local languages. Nigeria has committed to a national rollout of the C‐IYCF program, starting in several Nigerian states where funding is secured. After consultations with both SPRING and UNICEF, the FMOH agreed to conduct an evaluation of the package, knowing that the findings— which will be shared both nationally and internationally—will inform future investments in C‐IYCF programming.1
The main purpose of this evaluation is to assess the effectiveness of the C‐IYCF Counselling Package at improving IYCF behaviors in an environment that supports its design, management, technical assistance, and monitoring, when adapted for the local context and implemented at scale.2 While this evaluation is not nationally representative, the findings should be useful for national level decision making in Nigeria. The results of the evaluation will also make an important scientific contribution to the field of nutrition, in which there is relatively little evidence on the impact of a large‐scale community‐based IYCF counseling intervention.
The objectives of the evaluation are to—
- Assess the environment or context in terms of how it enabled or hampered the success of the implementation of the C‐IYCF Counselling Package in Kaduna state, Nigeria.
- Assess C‐IYCF Counselling Package program processes, implementation achievements, and costs.
- Evaluate the outcomes, after implementing the C‐IYCF Counselling Package, on counseling and communication skills and knowledge of IYCF among CVs.
- Establish the impact of implementation of the C‐IYCF Counselling Package on caregivers’ knowledge, attitudes, beliefs, and practices related to IYCF.
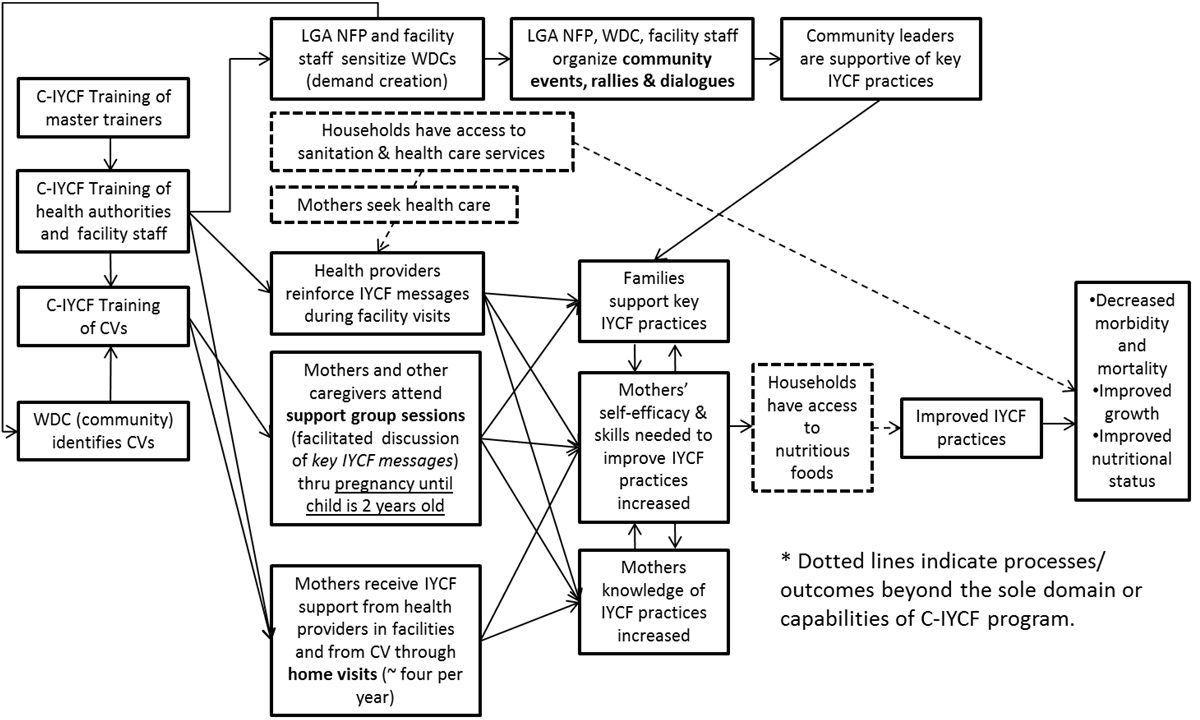
Figure 1: C‐IYCF Program Impact Pathways
Location
The evaluation is being conducted in one intervention local government area (LGA) and one comparison LGA in the state of Kaduna. Kaduna was selected based on the following inclusion criteria:
- limited intensive community‐based nutrition interventions
- very limited exposure to IYCF counseling and communication
- severe food insecurity is not a major factor
- socially stable environment is free of civil unrest
- willingness and commitment of community leadership to support and facilitate the implementation of the C‐IYCF Counselling Package.
Kajuru will be the intervention LGA. The comparison LGA will be Kauru; it was selected because of its similar geographic and socio‐demographic characteristics to Kajuru. The FMOH plans to implement the C‐IYCF Counselling Package in the comparison LGA after the endline is complete, estimated for late 2016 or early 2017.
Evaluation Design
The evaluation will follow a quasi‐experimental design and will use a mixed‐method approach for answering the research questions. Using several different data collection methods, described below, quantitative and qualitative data will be collected at baseline and endline, 18 months after the start of program implementation. While the facility assessment, the semi‐structured interviews, and the survey of CVs and health workers will be longitudinal (i.e., every attempt will be made to follow the same individuals at baseline and endline), the maternal survey will capture repeated cross‐sectional samples of pregnant women and mothers/caregivers of children under 2 years of age.
Intervention

After the baseline assessment is completed, the Kaduna State Ministry of Health (SMOH) and Kajuru LGA, with support from UNICEF/Nigeria, will implement the C‐IYCF program. A fundamental consideration for this evaluation is the sustainability and scalability of the intervention. As such, cost containment and local ownership
and responsibility are key. In addition, the intervention will be implemented with minimal outside funding, it will build on the established health and community systems. UNICEF will cover the cost of trainings, as well as the snacks and transportation to and from the meetings.
Progress to Date
Since September 2014, the evaluation has moved quickly. The protocol and data collection tools (semistructured interviews with federal, state, LGA, community, and health‐facility leaders; as well as the maternal survey) were submitted to John Snow, Inc.’s Institutional Review Board (IRB) and the National Health Research Ethics Committee of Nigeria (NHREC) in October. Approval was granted in early December. In addition, SPRING contracted with a local study coordinator, Susan Adeyemi, who began work in November.
Data Collection, Entry, and Analysis
In December 2014, the study coordinator, Ms. Susan Adeyemi; the co‐principal investigator (PI), Dr. Sascha Lamstein; and a small team of data collectors completed an assessment of the enabling environment. Ms. Adeyemi interviewed federal, state, and LGA stakeholders. Dr. Lamstein assisted with the federal‐level interviews. See annex 1 for a complete list of the agencies and institutions interviewed. In addition, eight data collectors were trained and conducted 51 health facility assessment key informant interviews and 78 interviews with community leaders in Kajuru (i.e., the intervention LGA).
In January 2015, Ms. Adeyemi, and Dr. Kolawole Oyediran (a SPRING consultant), trained 32 data collectors to administer the maternal survey tool to pregnant women and mothers of children under 2 years of age. Between mid‐January and mid‐March, 176 enumeration areas (EA) were randomly sampled in Kajuru LGA; and a total of 660 pregnant women and 1,820 mothers of children under 2 years were interviewed. In Kauru LGA (i.e., the comparison LGA) another 177 EAs were randomly sampled and a total of 1,025 pregnant women and 1,883 mothers of children under 2 were interviewed. The team decided to take anthropometric measurements for a sub‐sample of respondents—approximately one out of every three respondents in the original sample. In Kajuru and Kauru, 60 EAs were sampled and, at each site, the team took anthropometric measurements for all pregnant women and children under 2.
The Nigerian National Bureau of Statistics (NBS) entered data collected from interviews with health facility key informants, Ward Development Committee (WDC) members, and community leaders in Microsoft Excel. Dr. Rafael Pérez‐Escamilla and Dr. Lamstein are currently analyzing the data in Washington, D.C.
Implementing the C-IYCF Counselling Package

Kaduna state and Kajuru LGA authorities have been sensitized and engaged in planning the implementation. Since September 2014, the team conducted a total of five sensitization and advocacy meetings. In November 2014, UNICEF and SPRING met with the Kaduna SMOH to discuss the evaluation and introduce the study coordinator—the SMOH indicated their support.
In December 2014, UNICEF, SPRING, and the SMOH met with Kajuru LGA authorities; later, they met with the Ministry for Local Government to present and gain support for implementing their plans and their partners’ roles. The Ministry for Local Governments allocated funds for supervising and monitoring the implementation of the counseling package in Kajuru LGA. The LGA authorities are currently developing a plan for monitoring and supervising the implementation process.
In February 2015, UNICEF and SPRING met with the SMOH and the Ministry for Economic Planning to continue discussing the implementation of the C‐IYCF Counselling Package. The SMOH reaffirmed their commitment to ensure the success of the implementation and evaluation. The Ministry for Economic Planning indicated their commitment to supporting the implementation process—it recently secured a budget line specifically for nutrition activities.
Finally, in March, the study coordinator met with the Kajuru LGA authorities and the Ward Focal Persons in the Kajuru LGAs. This set the stage for recruiting and training the CVs for the C‐IYCF activities.
Finally, UNICEF printed the materials and master trainers (MTs) were contracted for the upcoming trainings of health workers and CVs.
Challenges

The scheduled elections and anticipated unrest delayed the data collection. Also, the political environment resulted in a hostile situation for the collection teams. Fortunately, in Kajuru LGA, with the support of community leaders, the data collection teams conducted the survey. However, in Kauru LGA, the team was met with hostility and could not conduct the survey in one of the randomly selected EAs, even though they had the community leaders’ support.
Data collection was further challenged by the difficult terrain and geographic isolation of the selected EAs, particularly in Kauru. This increased the travel time between EAs and, ultimately, the duration of the data collection.
Next Steps: April—June 2015
The NBS will complete data entry for the maternal survey by mid‐April, and a draft baseline report will be circulated in May 2015. After unrest or risk of unrest from the elections subsides, the team will complete the data collection:
- Study coordinator, Ms. Adeyemi, will work with Dr. Oni of UNICEF/Kaduna to engage the WDC in nominating CVs.
- In mid‐April, SPRING/UNICEF‐trained MTs will train approximately 100 health authorities and workers from Kajuru public primary health centers that have at least one person on staff.
- Following the training of the health workers, the team will hold an orientation meeting with the nominated CVs. Trained data collectors will conduct baseline (pre‐training) interviews with the CVs.
- In May, MTs and trained health workers will train approximately 250 CVs.
- Following this round of trainings, CVs will be invited to health facilities for a planning meeting. Again, a post‐training interview will be conducted with CVs at this time.
- Community‐based activities are expected to begin by June 2015.
Footnotes
1 The Principal Investigators (PI) of this evaluation are Rafael Perez-Escamilla of Yale University, consultant to SPRING, and Sascha Lamstein of SPRING. The co-investigators include Peggy-Koniz-Booher (SPRING), France Begin (UNICEF), Arjan De Wagt (UNICEF), Christine Kaligirwa (UNICEF), Babajide Adebisi (SPRING), and Chris Isokpunwu (FMOH). In addition, this work would not have been possible without the the support of Stanley Chitekwe, Davis Omotola, and Florence Oni of UNICEF, and the efforts of Susan Adeyemi, Emily Stammer, and Sarah Cunningham of SPRING.
2 Note that “scale” is defined as a local government area (LGA), a geographic area and population considered adequate for assessing replicability and generalizability to implementation at the national level.