April–December 2015

This progress report is part of the evaluation of Nigeria’s Community Infant and Young Child Feeding (CIYCF) Counselling Package, a joint endeavor of the Federal Ministry of Health (FMOH) of Nigeria, the United Nations Children’s Fund (UNICEF), and the Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project. By the end of 2014, 44 countries had adapted the C‐IYCF Counselling Package to their setting, building capacity and rolling out community‐based IYCF programming. Despite global interest in the C‐IYCF Counselling Package, little is known about its impact on maternal, infant, and young child nutrition (MIYCN) practices in the countries where it has been adapted. Therefore, high‐quality studies assessing the package’s effectiveness and impact are needed.
Nigeria offered us a unique opportunity to address this major gap in global evidence. With support from UNICEF and two USAID‐funded global nutrition projects—the Infant and Young Child Nutrition Project (IYCN) and SPRING—the FMOH has made a significant investment to adapt the UNICEF generic C‐IYCF Counselling Package to the Nigerian context, including translating it into six local languages. Nigeria has committed to a national rollout of the C‐IYCF program, starting in several Nigerian states where funding has been secured. After we consulted with both SPRING and UNICEF, the FMOH agreed to conduct an evaluation of the package, knowing that the findings—which we will share both nationally and internationally—will inform future investments in the C‐IYCF Counselling Package.1
This mixed methods evaluation assesses the effectiveness of the C‐IYCF Counselling Package when it is adapted for the local context and implemented at scale2 in one local government area (LGA) and in an environment that supports its design, implementation, and monitoring. More specifically, the primary aims of the evaluation are to—
- assess the environment or context in terms of how it enabled or hampered the success of the C‐IYCF Counselling Package
- assess the C‐IYCF program processes, implementation achievements, and costs
- evaluate the outcomes of the C‐IYCF Counselling Package on counseling and communication skills and community volunteers (CV) knowledge of MIYCN
- establish the impact of the C‐IYCF program on caregivers’ knowledge, attitudes, beliefs, and practices related to MIYCN.
We are conducting the evaluation in one intervention LGA (Kajuru) and one comparison LGA (Kauru) in Kaduna State. Planning for this evaluation began in April 2014. On‐the‐ground data collection began in December 2014.
This update includes information on recent activities, key findings to date, recommendations for rolling out the C‐IYCF Counselling Package, and next steps for the evaluation team. See the evaluation webpage for this information and more.
Recent Activities
In the last six months, much has happened with the data collection, data entry, data analysis, and program implementation.
Baseline Data Collection, Entry, and Analysis
Following the training of data collectors, the in‐depth interviews with key stakeholders from the enabling environment, and a maternal survey, we oversaw the management, entry, and analysis of baseline data:
- Enabling environment assessment: We analyzed the data from interviews with key stakeholders from the enabling environment—including federal, state, and LGA authorities; community members; and health facility staff members—in MS Excel and STATA version 13.1. The study coordinator translated the open‐ended responses. In early 2016, we will disseminate a report of the findings. See below for a summary of the key findings.
- Maternal survey: Twenty‐five trained3 data entry clerks entered data from the maternal survey into the SurveyCTO Application. The study coordinator, a coordinator recruited by the National Bureau of Statistics (NBS), and the UNICEF nutrition data manager, supervised the data entry process. The study coordinator, and the coordinator recruited by NBS, also conducted a random spot check of 10 percent of the entered data. Because of some challenges with the data entry process, data was not completed until early November 2015. We have almost completed the data analysis.
- Anthropometric sub‐sample survey: To complement the maternal survey, we also measured the anthropometry to assess the general nutritional status of pregnant women, children under two years, and their mothers. One‐third of the enumeration areas (60 in each LGA) included in the maternal survey were sampled for the anthropometric survey. Data were entered with the maternal survey data and the analysis is nearly complete.
- Pre‐and post‐training tests: Prior to and after trainings on the C‐IYCF Counselling Package, the health facility staff, health authorities, Ward Development Committee (WDC) members, and community members nominated to serve as CVs were assessed on knowledge, attitudes, and practices (KAP) related to MIYCN. Five trained data entry clerks used a double data entry process to enter data into CSPro. In addition, the study coordinator conducted random spot checks of entered data. STATA version 13.1 was used to analyze the data. As mentioned previously, the study coordinator translated the open‐ended responses. A report of the findings is being prepared and should be circulated in January 2016.
Implementation of the C-IYCF Counselling Package

Implementing the C‐IYCF Counselling Package in Kajuru LGA includes (1) sensitizing the key stakeholders, (2) selecting and training the health facility staff, (3) nominating and training the CVs, (4) forming support groups, (5) conducting support groups and home visits, (6) sensitizing and mobilizing community members, (7) monitoring, and (8) conducting monthly review meetings and supportive supervision for CVs and health workers. Between June and December 2015, we completed the following related activities:
- Prepared the C‐IYCF master trainers: In May, UNICEF Nigeria organized a one‐day training on the C‐IYCF module “Supportive Supervision/Mentoring and Monitoring for Community IYCF” for nine C‐IYCF master trainers.
- Advocacy and sensitization visits: Beginning in November 2014, UNICEF, SPRING, and the Kaduna State Ministry of Health (SMOH) conducted numerous advocacy visits with key stakeholders from the Kaduna State government (e.g., the Ministry of Local Government, the Ministry of Chieftaincy Affairs, and the Ministry of Planning) and the Kajuru LGA, as well as with community leaders, particularly WDC members. To be effective, these visits must be made periodically, or when staff turns over in the LGA or state government.
- Selection and training of health facility staff: In May 2015, we trained nurses, community health extension workers (CHEW), junior CHEWs, and community health officers that worked in aPHC in the intervention LGA that met the following criteria: (1) provides child welfare/antenatal care services, (2) has a minimum of two posted health personnel, and (3) has no current staff trained in the package. In addition, we trained LGA authorities. In total, 86 people were trained during four six‐day trainings led by master trainers using the “Training of Coaches & Supervisors” and the “Supportive Supervision/Mentoring and Monitoring for Community IYCF” modules.
- Nomination and training of CVs: In consultation with health facility staff, WDC members nominated 239 community members to serve as CVs in the 10 wards of Kajuru LGA. This number of CVs would achieve a ratio of one CV per 40 children under the age of two. WDCs and community leaders nominated community members who were (1) willing to serve as CVs; (2) interested in breastfeeding, child feeding, child care, and community service; (3) able to read and write or access to someone who can; (4) of reproductive age (parents were preferred); and (5) speak the local language. All but one person nominated to serve as a CV were trained by master trainers and trained health facility staff during 10 three‐day trainings conducted in June 2016.
- Community dialogs were conducted for one day in each of the 10 wards, with a total of 400 people attending, including traditional and religious leaders. Subsequently, 2,000 community members were sensitized and the platform was established for implementing the C‐IYCF in Kajuru.
- Formation of support groups: Following the training and the post‐training survey of CVs, and with help from health facility staff and WDC members, CVs formed 257 support groups.4 This identified the pregnant women and mothers of children under two.
- Harmonization of monitoring tools and processes: The evaluation team, including representatives from UNICEF and SPRING, participated in an effort to harmonize the C‐IYCF monitoring tools used nationwide by government and nongovernmental agencies.
- Monitoring and review: During the training, CVs were taught to use the C‐IYCF Counselling Package registers and reporting forms. CVs are successfully completing their monthly reports. They are submitted to health facility staff and reported during monthly review meetings that began at the end of August 2015 and are held in local facilities. The LGA nutrition focal person (NFP), state nutrition officer (SNO), and assistant state nutrition officer (ASNO), with support from the study coordinator, organize and lead these meetings.
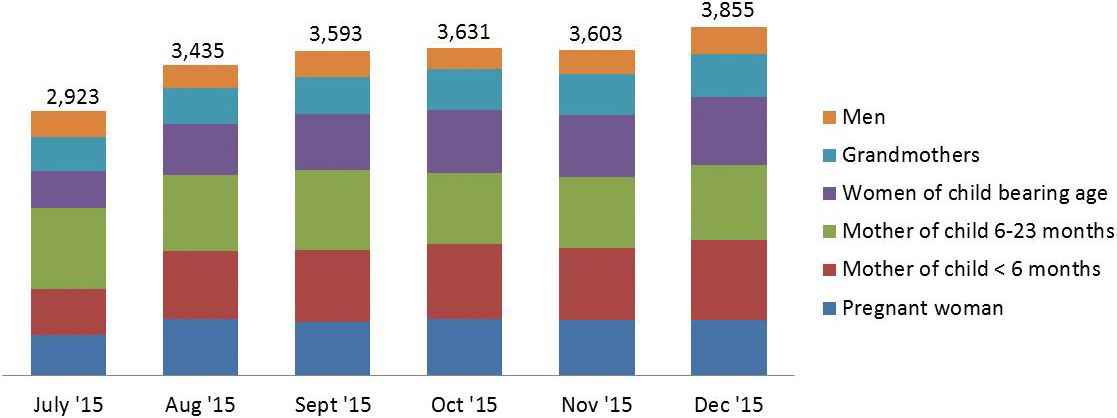
- Conducting support groups and home visits: Using the monitoring forms completed and submitted during the review meetings, we are pleased to report the successful implementation and impressive reach (see table below). To date, 297 support groups have been formed and 11,008 support group meetings were held, with a total of 13,582 contacts made. The majority of participants were mothers of children 6–23 months old, mothers of children under six months old, pregnant women, and other women of reproductive age. In addition, 1,770 home visits were made and 249 people were referred to the health facility for additional care.
- Supportive supervision: The Kaduna SNO or ASNO, with the Kajuru LGA NFP, are committed to conducting routine supportive supervision visits. In turn, trained health facility staff are committed to supporting CVs by attending support groups and coaching CVs on topics and techniques. To date, PHC staff conducted 509 supportive supervision visits to CVs and the Kajuru LGA NFP, the UNICEF/Kaduna nutrition specialist, and/or the study coordinator conducted another 12. Most CVs had at least one supportive supervision visit.
Figure 1. Number of People Who Attended Support Group Meetings, by Month and Type if Participant
Summary of Findings to Date
Our findings from the enabling environment assessment—in‐depth interviews at the federal, state, LGA, health facility, and community levels—suggest strong support for deploying the MIYCN programs like the C‐IYCF Counselling Package, as well as several areas for improvement, as indicated below:5
- Policies affect food, care, and health, although their impact varies, based on adherence and enforcement. For example, policies regarding breastfeeding such as the “National Policy on Infant and Young Child Feeding in Nigeria,” affect the promotion of breastfeeding among health workers and other health authorities. While, at the national level, most policies were available; at the state level and below, nutrition‐related policies, reports, and tools were rarely available, even within the SMOH. Federal offices represented were strongly engaged with federal‐level policies and programs and overseeing the work of state‐level offices; however, nothing indicated that they were heavily involved in reviewing data related to MIYCN.
- Governance, which refers to participation, accountability, and voice, also impacts a country’s progress toward good nutrition. According to the Fifth Report on the World Nutrition Situation by the United Nations Standing Committee on Nutrition, to address malnutrition effectively requires effective governance systems6. An important starting point for good governance and management is the agenda‐setting, or prioritization process. Interviews conducted at the federal level found little evidence of inter‐ministerial coordination for decisions regarding administration and implementation of MIYCN programs. Some evidence suggests that systems are quite segmented, even among units within the same ministry. Furthermore, respondents explained that decisions at the state level are strongly influenced by national priorities, which are established through a silo system, further confirming the lack of multi‐sectoral or inter‐ministerial coordination. Interviews also suggested the limited engagement of representatives from the state, LGA, health facility, and community levels in setting the agenda or planning the implementation. While state offices were strongly engaged with budgeting and oversight of state‐level policies, and programs were engaged at the LGA level, we did not find any evidence that they were engaged at the community level.
Governance is also about implementing interventions. CVs play an essential role in the C‐IYCF Counselling Package program implementation. Prior to training, those nominated to serve as CVs in Kajuru LGA were surveyed. Our findings are useful for assessing the effectiveness of the trainings at a later data and gaining a better sense of how prepared the nominated CVs are to serve in that role. Our findings also suggest that those nominated to serve as CVs generally meet the established criteria. However, they also indicate the need to bolster their MIYCN knowledge and attitudes, as well as their decision‐making power, agency, and mobility to ensure that they can effectively and confidently carry out their responsibilities. - In terms of resources, we did not look closely at the budget allocations for IYCF at this time. However, it is an area that we will explore going forward. We found that human resources at the health facilities in the intervention LGA were severely inadequate, which limited their ability to supportively supervise CVs, which would ensure the quality of C‐IYCF program implementation.
- Social norms and social support can also affect the success of any program, particularly if they involve behavior change. For women to adopt optimal maternal and IYCF practices, husbands, mothers‐in‐law, and community leaders—including WDC members, as well as health facility and LGA staff—will need to support the adoption of those practices. While respondents at all levels understood the need for maternal and IYCF programming—and federal, state, and LGA representatives expressed wiliness to actively support the program—we found that health facility staff were ambivalent about their role in working with and supporting CVs. They mentioned a lack of funding, little community engagement, and a negative perception of the role of CVs in the community.
- CVs play a fundamental role in implementing the C‐IYCF Counselling Package. Indeed, without CVs, the interventions would not happen. Therefore, social norms and perceptions related to CVs is an important consideration. We recommend that emphasis be placed in highlighting the potential for the whole health care system—specifically the health of women, young children, and their families—when they have a well‐trained and supervised cadre of MIYCF CVs.
Knowledge of maternal and IYCF practices was reasonably good at the national, state, LGA, and facility levels, but we found that room for improvement was obvious, particularly the importance of not giving any water or pap before 6 months of age and continuing breastfeeding for two years. However, among WDC members and community leaders, knowledge was suboptimal, suggesting a need for training them, as well as the CVs. Furthermore, responses from key informants, at all levels except the national level, suggested that women’s decision‐making ability may be limited, particularly as it relates to maternal and IYCF practices. This was especially visible at the community and health facility level. We are concerned because the IYCF program relies heavily on women having a critical amount of social support and autonomy in the decision‐making process regarding their health and that of their family members, including her young children. Thus, it is important to sensitize facility, community, ward, and LGA leaders on the importance of and need for women’s empowerment.
Respondents from various levels of the enabling environment told us they were not confident that all target populations would participate in support groups, particularly newly married women, mothers‐in‐law, and other relatives. This may be the result of either the lack of prior experience with IYCF‐like support groups, or perhaps with previous negative experiences organizing support groups for health education purposes. We expect this perception may change with their direct experience after the C‐IYCF program is implemented in Kaduna.
Findings suggest that the implementation of the C‐IYCF program will need to strengthen the enabling environment from the perspective of a multi‐level system.
Considerations for Implementation of the C-IYCF Counselling Package

Based on these initial findings, we suggest that the following activities be considered to strengthen the enabling environment and ensure optimal implementation:
- Organize routine coordination meetings, at all levels, to strengthen intersectoral participatory coordination for implementing the C‐IYCF Counselling Package.
- Distribute key policy and program documents, as appropriate, to state, LGA, and health facility staff.
- Conduct ongoing sensitization of decision makers, at all levels, about the strong potential that CVs have to deliver nutrition programs, the need to identify and provide sustainable incentives for the CVs, and the important role of women in decisions related to MIYCN practices.
- Pay attention to the self‐esteem, self‐efficacy, and agency of CVs to ensure they can carry out their responsibilities.
- Organize workshops and/or seminars for federal and state officials to increase their knowledge of MIYCN practices.
- Encourage the LGA NFP to support the health facility staff and CVs, technically and administratively, through supportive supervision visits.
- Advocate for increased funding for supportive supervision of C‐IYCF program activities.
- Engage health facility staff in decisions regarding the design and implementation of the C‐IYCF program and in agenda setting to improve MIYCN practices.
- Discuss and implement strategies to incentivize non‐pregnant women, husbands, mothers‐inlaw, and other relatives who might influence IYCF practices to participate in C‐IYCF program activities.
Next Steps for the Evaluation Team
Over the next six months, we plan to complete the following activities:
- Complete the analysis and reporting of baseline findings from the maternal survey, anthropometry sub‐sample survey, and pre‐and post‐training tests/surveys.
- Complete the routine satisfaction surveys for the CVs and C‐IYCF program beneficiaries.
- Complete the mid‐course on‐site assessment of fidelity to C‐IYCF program implementation plans (tentatively planned for March–April 2016).
Footnotes
1 The Principal Investigators (PI) of this evaluation are Rafael Perez-Escamilla of Yale University, consultant to SPRING, and Sascha Lamstein of SPRING. The co-investigators include Peggy-Koniz-Booher (SPRING), France Begin (UNICEF), Arjan De Wagt (UNICEF), Christine Kaligirwa (UNICEF), Babajide Adebisi (SPRING), and Chris Isokpunwu (FMOH). In addition, this work would not have been possible without the the support of Stanley Chitekwe, Davis Omotola, and Florence Oni of UNICEF, and the efforts of Susan Adeyemi, Emily Stammer, and Sarah Cunningham of SPRING.
2 The research team defined at scale as a geographic area and a population large enough for them to assess the replication of the program at the national level. It was agreed that one intervention LGA with a population of more than 140,000, and a goal to cover 100 percent of the mothers of children under two, would be sufficient.
3 UNICEF nutrition data manager, supported by NBS, held a special one-day training on this large dataset for the data entry clerks.
4 CVs were advised to allow no more than 12 people in each support group. As attendance increases, they should form new support groups. By the end of October 2015, 297 support groups had been formed, reflecting the increased attendance.
5 The complete report will be circulated in early 2016.
6 ACC/SCN. 2004. “Fifth Report on the World Nutrition Situation: Nutrition for Improved Development Outcomes.” Geneva, Switzerland: Administrative Committee on Coordination/Subcommittee on Nutrition of the United Nations (ACC/SCN).