The “Great SBCC Example” below was featured during the Designing the Future of Nutrition Social and Behavior Change Communication Conference and can be used as a learning aid or as an illustration of key concepts from country-level experts attending the conference.


Background
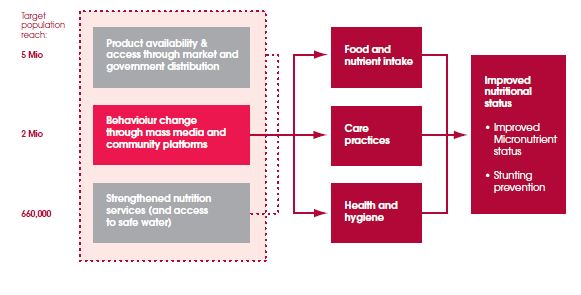
Sidoarjo in East Java province is a region of Indonesia where overall child nutrition is quite poor. The Global Alliance for Improved Nutrition (GAIN) is implementing an integrated approach to stunting reduction that includes access to nutritious foods and supplements, access to safe drinking water, better hygiene practices, and health systems strengthening, as well as a large behavior change component promoting appropriate feeding practices for children under two years of age and improved maternal nutrition.
Description of Intervention
The intervention uses mass media, including television commercials, and community mobilization through social activities centered on women’s groups. The behavior change component focuses on three key feeding behaviors for children under two, using multiple channels: mass and social media, community activation and interpersonal counseling in the health center. The mass media campaign theme is built around a social activity common in the communities, sharing chitchat or gossip. The main characters are (a) the ”gossip lady,” a silly but lovable character who always comments on the behavior of other mothers, (b) key authority figures such as grandmothers or midwives, and (c) the good mother, who is targeted by the gossip lady but actually demonstrates the good nutrition-related behaviors that need to be promoted.
Design Process
The intervention design was based on a theoretical framework developed by the London School of Hygiene & Tropical Medicine (LSHTM). The formative research methodology relies in part on extended observation of participants—in the present study this was conducted by video in participants’ homes. This method allowed the capture of participants’ observable behavior as well as their reported actions. Findings identified the need to focus on three key behaviors and use non-conscious motives to help drive change in these behaviors.
Findings on infant and young child feeding and related behavioral insights were used to structure a creative brief for development of a campaign theme, three TV commercials, and a community activation program. A creative marketing agency translated the insights into an aspirational concept, which was pre-tested before the mass media campaign plan was finalized and community intervention begun.
During the creative design process, the GAIN project design team collaborated with the academic team of the LSHTM and the design team of Playgroup, an Indonesian commercial creative agency. This multidisciplinary team—despite posing some challenges—guaranteed a rich, interactive, and imaginative process. The academic team provided careful scrutiny of proposed storyboards and creative strategies to ensure that behavior change principles were consistently applied and translated into creative solutions. The creative team used their extensive knowledge of the Indonesian culture and context to ensure grounding of formative research insights and behavior change principles in a lively and socially appropriate narrative.
Design Constraints
Health professionals often lack the skills, tools, or time to provide nutritional guidance to patients and community members. On the other hand, formula manufacturers use large marketing budgets to wield undue influence and enforcement of national regulations governing the marketing of breast milk substitutes is weak.
Design Strategies
The intervention was designed to respond to the findings of formative research, including these insights:
- Knowledge about nutrition is important but insufficient to lead to change: Mothers were familiar with the key messages of “breast is best” and “diverse diet.” But they did not necessarily understand or believe the information behind these slogans, nor act on it.
- Confidence is crucial: Many mothers lack confidence in their own ability to breast-feed or in the quality or quantity of their breast milk, which leads to the introduction of formula, or in their ability to make the right choices. Their uncertainty means that well-intended advice can lead to undesired behavior such as early introduction of formula and/or complementary foods.
- Some parents act on a belief that the baby knows best: A parent’s focus on nurturing their baby can turn into an effort to soothe the child rather than provide for nutritional needs. Parents often respond immediately to their children’s demands by pacifying them, providing unhealthy snacks or bottled milk, even close to mealtime. Parents may find unhealthy children’s snacks appealing because they are sold in convenient individual portions that avoid the wasting of food—and mothers do not need to involve themselves in feeding a child as soon as the child can reach the food and feed itself.
- Peer influence can have a negative influence: Family, friends, and neighbors affect child feeding behavior, often offering morsels of food to “help” quiet the baby.
Implementation Strategies
- Focus on building mothers’ confidence and establishing new social norms, by using key authority figures to correct the incorrect behavior and validate the desired behavior.
- Present strong visual rejection of the incorrect behavior (such as slapping away the feeding bottle) and visual demonstration of the desired behavior (breastfeeding).
- Focus on a few clearly defined complementary feeding behaviors instead of knowledge (discourage introduction and use of infant formula; increase dietary quality and diversity of the family meal plate by reducing the proportion of rice [same foods, different portions] ; and reduce unhealthy snacks before meals.).
- Address social norms and the influence of key authority figures on mothers and caregivers.
Evidence of Effectiveness
The behavior change communication component reached 2.5–3 million people through TV commercials and 60,000 people through community mobilization activities. Interpersonal communication reached more than 10,000 mothers with children under two years and an additional 15,000 mothers of children aged two to five years.
Key Takeaways for Nutrition Social and Behavior Change Communication
- Focus on non-conscious motives for behavior: A new theoretical framework and formative research methodologies provided key insights, which also revealed some of the important non-conscious drivers of behavior (e.g., status and affiliation).
- Focus on fewer behaviors to achieve greater impact: Formative research, together with stakeholder input, prioritized three feeding behaviors.
- Engage in effective multisectoral partnerships: Intervention design development and execution involved a diverse group of experts, including private sector creative talent, academic experts, field researchers, and government representatives.
- Capitalize on local and commercial expertise: This helped shape design principles for the TV commercials:
- “Keep it real”: Use real-life dialogue, portraying everyday situations and realistic actions, and avoid using a lecturing tone or public health jargon.
- Use visual demonstration: Show both the incorrect and desired behaviors in action, followed by a reward for the correct behavior in the form of approval by the key authority figure or a smiling baby.
- Confirm a social norm: Make the target behavior appear common across the population.
- Ensure "stickiness” of the TV commercials and key messages: Use attention-grabbing, funny gestures or sounds that are funny or a bit cheeky.
Organizations: GAIN and the London School of Hygiene & Tropical Medicine, Hygiene Centre
GAIN is an international foundation driven by the vision of a world without malnutrition. It acts as a catalyst—building alliances between governments, business, and civil society—to innovate and deliver solutions for impact at scale. The London School of Hygiene & Tropical Medicine is a world-leading center for research and postgraduate education in public and global health. The Hygiene Centre is a multidisciplinary group dedicated to improving hygiene and sanitation.