Overview of the Global Anemia Problem, Including Iron Deficiency Anemia
The World Health Organization (WHO) defines anemia among women of childbearing age as the condition of having a hemoglobin concentration of < 12.0 g/dL at sea level; among pregnant women it is defined as < 11.0 g/dL. The hemoglobin concentration cutoff level that defines anemia varies by age, gender, physiological status, smoking status, and the altitude at which the assessed population lives.
The primary cause of anemia is iron deficiency, a condition caused by inadequate intake or low absorption of iron, the increased demands of repeated pregnancies—particularly if not well spaced (e.g., fewer than 36 months between pregnancies)—and loss of iron through menstruation. Other causes of anemia include vitamin deficiencies (such as a deficiency of folic acid or vitamin A), genetic disorders, malaria, parasitic infections, HIV, tuberculosis, common infections, and other inflammatory conditions. While iron deficiency anemia (IDA) accounts for about onehalf of all anemia cases, it often coexists with these other causes.
Iron deficiency anemia is most common during pregnancy and in infancy, when physiological iron requirements are the highest and the amount of iron absorbed from the diet is not sufficient to meet many individuals’ requirements (Stoltzfus and Dreyfuss 1998). Anemia’s effects include increased risk of premature delivery, increased risk of maternal and child mortality, negative impacts on the cognitive and physical development of children, and reduced physical stamina and productivity of people of all ages (Horton and Ross 2003). Globally, IDA annually contributes to over 100,000 maternal deaths (22 percent of all maternal deaths) and over 600,000 perinatal deaths (Stoltzfus, Mullany, and Black 2004). Key anemia control interventions include promoting a diversified diet, iron-folic acid (IFA) supplementation during pregnancy, iron fortification of staple foods, prevention and treatment of malaria, use of insecticide-treated bed nets, helminth prevention and control, delayed cord clamping, and increased birth spacing.
Maternal Anemia in Zambia
According to the most recent and available data— now more than a decade old—the prevalence of anemia among pregnant women in Zambia is 47 percent, making it a severe public health problem as defined by WHO standards1 (Luo, Mwela, and Campbell 1999). In terms of anemia severity, severe anemia (hemoglobin < 7.0 g/dL) among pregnant women in Zambia may have multiple causes. A 1989 study among pregnant women in the city of Ndola found that malaria and hookworm infections, as well as iron and folate deficiency, were associated with severe anemia (Fleming 1989). Although the study is dated, areas in Zambia in which one or more of these potential causes are prevalent may be expected to show a high prevalence of anemia as well.
Falter Points in Women's Consumption of Iron-Folic Acid During Pregnancy
WHO recommends that all pregnant women receive a standard dose of 30–60 mg iron and 400 μg folic acid beginning as soon as possible during gestation (WHO 2012). Ideally, women should receive iron-containing supplements no later than the first trimester of pregnancy, which means ideally taking 180 tablets before delivery. It is important to note, that many countries aim for women to receive 90 or more tablets during pregnancy.
Figure 1 shows a decision-tree analysis of how well the Zambian antenatal care (ANC) system distributes IFA, and identifies four potential points at which the system might falter (highlighted in orange). The figure tracks the number and percentage of women who obtained ANC, those who subsequently received and consumed at least one IFA tablet, and those who consumed the ideal minimum number of tablets.2All data are based on Zambia Demographic and Health Survey (ZDHS) questions asked of women who were in permanent unions and had been pregnant in the five years prior to being interviewed3 (CSO et al. 2009).
Figure 1. Analysis of Falter Points Related to Distribution and Consumption of IFA through Zambia’s ANC Program in 2007, Women of Reproductive Age (15–49 years) n=7,146
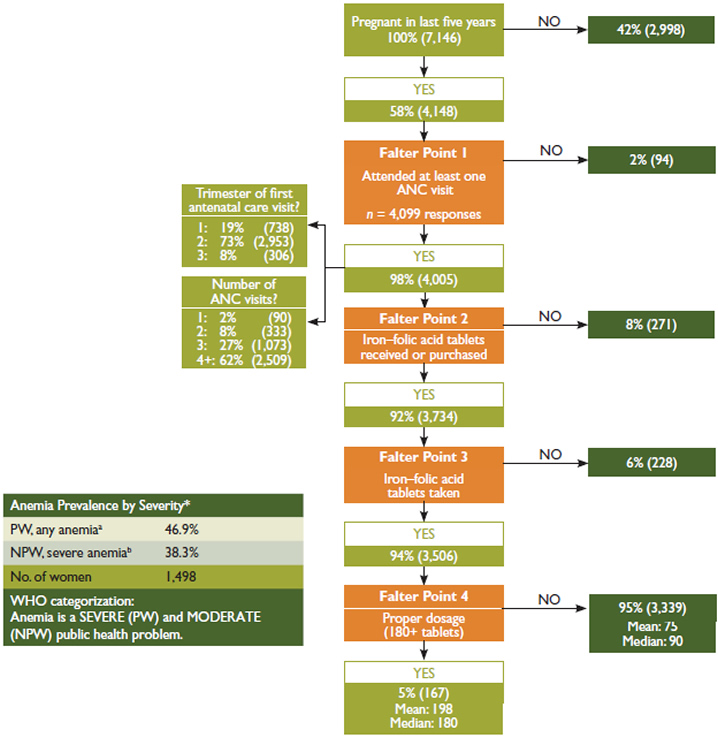
Main Conclusions: Given the high coverage rate, ANC provides an outstanding platform for distributing IFA. Among women who were pregnant in the last five years, had at least one ANC visit, and took at least one IFA tablet, only five percent received and took the ideal minimum number of tablets. Falter Point 4 is the most critical shortcoming within the system, followed by Falter Points 2 and 3. Both supply and demand are likely constraints.
Percentages are calculated from weighted data and may vary slightly from the unweighted observations-based calculations. One percent of women who were pregnant in the last five years did not have any ANC visits but received or purchased IFA from another source.
*Percentage of women 15–49 years based on Hemoglobin levels, Hb (g/dL)
aNPW 10.0≤Hb≤11.9, PW 10.0≤Hb≤10.9 b7.0≤Hg<9.9 cHg<7.0
Non-responses, no data (NR/ND) were recoded to “No” for “At least one ANC visit?”, “IFA tablets received?”, and “IFA tablets taken?” and to zero for “Number of tablets taken?”.
Anemia prevalence data are provided as a reference point, signaling the general order of magnitude of the anemia public health problem. The ANC utilization data is based on self-reported data of women 15–49 years in permanent unions and pertains to their last pregnancy in the last five years prior to the DHS.
Source: Calculations are from the Zambia Demographic and Health Survey (2007). Anemia levels are from the WHO VMNIS, Reference 2477, 1998.
Many supply-side aspects—including both adequacy of IFA tablet supplies and technical knowledge and practices of ANC providers—need to be considered when assessing how well an ANC program delivers IFA. In addition, as Falter Point 4 in Figure 1 clearly shows, the provision of IFA tablets to a pregnant woman is a necessary but not sufficient condition for the woman to consume the tablets, particularly at the ideal minimum level. Thus, demand-side factors also play a critical role in determining the coverage and effectiveness of a program. These include whether or not women seek ANC and the timing and number of visits, as well as the extent to which women are aware of the significance of anemia and IFA, ask for IFA tablets, and comply with the IFA regimen.
Understanding the relative significance of each falter point makes it possible to prioritize them for more in-depth analysis, providing a first step in an evidence- based approach to systematically improving the program. The DHS does not collect information on the number of IFA tablets received by women. In the case of Falter Point 4, this lack of data creates ambiguities that make it impossible to fully understand whether shortcomings of the system relate primarily to supply- or demand-side factors. Despite this limitation, the decision-tree analysis presented in Figure 1 still enables prioritizing the falter points for more in-depth analysis and action at the national, district, and health center levels.
Analysis of Falter Points
Falter Point 1:
Did not attend at least on ANC visit
Only two percent of women did not have at least one ANC visit.
ANC’s high coverage gives it great potential as a vehicle for providing IFA.
Falter Point 2:
Did not receive or purchase at least one IFA tablet
Of the women who had at least one ANC visit, eight percent did not receive or purchase any IFA tablets.
This supply-side constraint is relatively small and may be due to various system/supply-side performance shortcomings, which could reflect: (1) inadequate supply (e.g., stockouts); (2) inadequate provider knowledge; or (3) inadequate provider practices, whereby IFA may not have been provided. As Figure 2 shows, this is the second-most important falter point among all pregnant women in Zambia.
Unfortunately, the ZDHS does not report the source(s) of the IFA tablets women received or purchased, and a small percentage of women attending ANC get IFA tablets from a different source. While only one percent of Zambian women who received or purchased IFA did not have any ANC visits (not shown), we cannot ascertain whether or not those who received ANC obtained their IFA from their ANC provider. However, women who attend ANC may be more likely to be aware of, to value, and also to take IFA tablets, regardless of where they obtain them. Thus, we would expect a high correlation between the number of women who had at least one ANC visit and those who received or purchased IFA, which is consistent with the data. Women who had one or more ANC visits and who did not receive any IFA represent a missed opportunity to reduce the risk of anemia among a high-risk population.
Falter Point 3:
Did not take at least one IFA tablet
Of the women who received IFA, six percent did not consume any tablets.
This demand-side constraint is relatively small and may be due to women not understanding the significance of anemia and/or the significance of IFA. This misunderstanding may reflect: (1) inadequate provider counseling and follow-up; (2) women’s beliefs about actual or possible side effects; or (3) sociocultural factors.
Falter Point 4:
Did not consume 180 or more IFA tablets
Of the women who received and took IFA, 95 percent did not consume the ideal minimum of 180 IFA tablets.
This constraint results from a combination of supplyand/ or demand-side factors. Figure 1 suggests two situations that may contribute to possible causes of this falter point: 81 percent of women who received ANC began their care after the first trimester, and the 37 percent who had fewer than WHO’s recommended four ANC visits during their last pregnancy may have started their ANC too late or may not have had enough visits to receive 180 tablets (given IFA distribution protocols). Both of these scenarios are likely contributors, but further research is needed to establish their relative importance, as well as the significance of other possible causes.
Globally, research has found that the following situations often contribute to Falter Point 4: (1) providers do not have access to adequate supply; (2) women do not receive adequate tablets because they have little access to care, start ANC late, or do not have enough ANC visits, making it difficult to obtain 180 tablets (given IFA distribution protocols); (3) providers do not provide adequate counseling or follow-up; (4) women do not adhere to the regimen, which may be due to difficulty in remembering to take the tablets daily, not knowing all the tablets are necessary, fear of having a big baby, side effects, or tablet-related issues (taste, size, color, coating, packaging/storage problem). Further research is needed to determine the underlying factors contributing to this falter point in Zambia.
Analysis by Sociodemographic Variables and Trends Over Time
A comparison of data from the 2001/2002 and 2007 ZDHS (Figure 2) highlights the great progress Zambia has made in improving IFA coverage and expanding its already high-performing ANC system. Ninety percent of women reported receiving and taking at least one IFA tablet during their ANC visit(s) in 2007, and the percentage of women taking 90 or more IFA tablets more than doubled over the five-year period. While this is encouraging, it is important to bear in mind that 90 tablets is merely one-half of the ideal minimum. Only 19 percent of women had their first ANC visit within their first trimester in 2007—an improvement, however, of 36 percent since 2001/2002. Continuing to increase this percentage will be critical to achieving an ideal minimum regimen of 180 IFA tablets taken throughout pregnancy.
A closer inspection of the number and timing of ANC (Table 1) reveals that although there was an overall decrease in the percentage of women receiving no ANC, the number of women having the WHO-recommended four or more visits dropped by 11 percentage points. With respect to the timing of ANC, more women are receiving ANC within the first two trimesters, and there has been a general decline in the percentage of women having their first ANC visit in the last three months of pregnancy.
Figure 2. Progress in ANC and IFA Indicators in Zambia, 2001/2002–2007
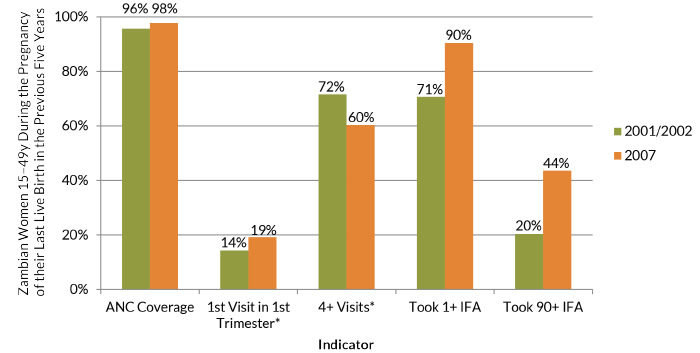
*Percentages among women who had at least one ANC visit.
Note: The 2001/2002 and 2007 ZDHS used an upper limit of 90-plus IFA tablets.
Table 2 disaggregates current ANC and IFA coverage (defined as the percentage of women, among all women who were pregnant in the past five years, who received and took at least one IFA tablet) rates by province, residence area, and wealth. Very minor differences in ANC coverage exist across the various characteristics, with more than 95 percent of women receiving ANC among all subgroups. This impressive level of equity in coverage is rare in low- and middle-income countries (LMICs). The most marked differences in IFA coverage are not by residence area or wealth, but by province. The percentage of women taking IFA tablets ranges from a low of 85 percent in the Eastern province to 96 percent in the Southern province.
Analysis by Geographic Region
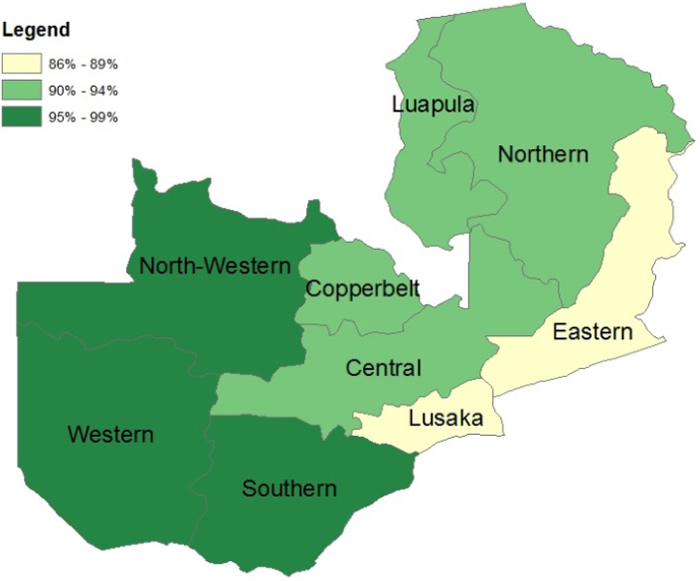
The map in Figure 3 shows the variation by province in the percentage of women who had at least one ANC visit and who received at least one IFA tablet. Through the ANC system, IFA coverage is high compared with other LMICs and little variation exists between provinces. Coverage ranges from 86–89 percent in Lusaka and the Eastern province, to 95–99 percent in the western-most provinces. Expanding ANC may assist in improving access to IFA and taking advantage of a missed opportunity to get more women to achieve an ideal minimum regimen of 180 tablets during their pregnancy.
Figure 3. Percentage of Women Who Had at Least One ANC Visit and Received at Least One IFA Tablet by Province, Zambia, 2007
Analysis by Number of ANC Visits
Figure 4 shows the relationship between the number of IFA tablets taken by women who had at least one ANC visit and the number of ANC visits they had during their last pregnancy. Forty percent of women who had at least one ANC visit took at most one-quarter (45) of the ideal minimum number of IFA tablets. While women with more visits were generally likely to receive and take more IFA tablets, the relationship is weak and not systematic. Additional ANC visits usually, but not always, result in modest increases in the number of IFA tablets consumed, underscoring the importance of the timing of the first ANC visit for achieving WHO standards. Only six percent of women who had four or more ANC visits received the ideal minimum number of IFA tablets. Learning what accounts for this ceiling is a critical challenge to improving the effectiveness of the ANCbased distribution of IFA in Zambia.
Table 1. Number and Timing of Antenatal Care Visits, Zambia, 2001/2002 and 2007
| Indicator | 2001/2002 | 2007 | Change in Coverage | Percentage Change |
|---|---|---|---|---|
| Number of ANC Visits | ||||
| Month of First Visit | ||||
| 0 | 4.1% | 2.1% | -2.0% | -48.8% |
| 1 | 2.0% | 2.3% | 0.3% | 15.0% |
| 2-3 | 19.8% | 34.0% | 14.2% | 71.7% |
| 4+ | 71.6% | 60.3% | -11.3% | -15.8% |
| Don't Know / No Data | 2.5% | 1.3% | -1.2% | -48.0% |
| No Antenatal Care | 4.1% | 2.1% | -2.0% | -48.8% |
| <4 | 14.3% | 19.2% | 4.9% | 34.3% |
| 4-5 | 52.4% | 53.4% | 1.0% | 1.9% |
| 6-7 | 26.7% | 23.2% | -3.5% | -13.1% |
| 8+ | 1.9% | 1.7% | -0.2% | -10.5% |
| Don't Know / No Data | 0.6% | 0.4% | -0.2% | -33.3% |
Overall Conclusions and Recommendations
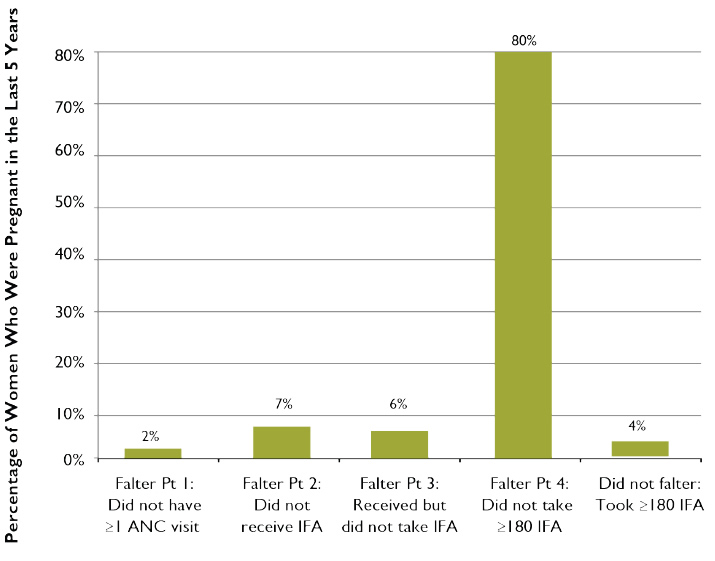
Figure 5 presents the obstacles among all women, including those who did not receive ANC during their pregnancy, to taking the minimum ideal number of IFA tablets. In Zambia, Falter Point 4 is by far the greatest barrier. Improving the delivery of IFA supplementation to Zambian women will therefore rely heavily on identifying and addressing program gaps in IFA supply management and health workers’ practices. Modifying some women’s long-term adherence behaviors, and addressing other points mentioned above under “Analysis of Falter Points,” may also lead to more women taking a minimum of 180 tablets (addressing Falter Point 4).
Receiving quality ANC is essential to achieving Millennium Development Goal (MDG) 5: improving maternal health and reducing maternal mortality. Zambia’s maternal mortality rate (MMR) is one of the highest in the world, at 483 maternal deaths per 100,000 live births, despite its high ANC coverage. Significant improvements must be made if the country is to meet its MMR target of 162.3 in 2015 (UNDP 2013). Zambia has outlined priority interventions for maternal health in its National Health Strategic Plan for 2011–2015. Included in its key strategies for integrated reproductive health within the Basic Health Care Package is the scale-up of IFA supplementation to pregnant women (MOH 2010). As this rapid assessment of the distribution of IFA tablets through ANC in Zambia suggests, there is substantial room for improving both the supply and the demand sides of the country’s ANC program. Improving the distribution of IFA through the ANC program is an important strategy for preventing and controlling anemia in Zambia, and for improving the nutrition and health status as well as the mental and physical capacity of women of reproductive age.
Table 2. ANC Coverage and IFA Tablets Taken During Last Pregnancy in the Last Five Years by Province, Residence and Wealth, Zambia, 2007
| Characteristic | No. Women with a Live Birth | Received ANC | Took 1 + IFA Tablet | ||
|---|---|---|---|---|---|
| Number | Percentage | Number | Percentage | ||
| Province | |||||
| Residence | |||||
| Wealth | |||||
| Central | 405 | 393 | 97.0% | 365 | 90.0% |
| Copperbelt | 606 | 597 | 98.5% | 555 | 91.6% |
| Eastern | 629 | 620 | 98.6% | 535 | 85.1% |
| Luapula | 346 | 336 | 97.1% | 315 | 91.1% |
| Lusaka | 520 | 519 | 99.8% | 463 | 89.0% |
| Northern | 629 | 612 | 97.3% | 564 | 89.6% |
| North-Western | 243 | 231 | 95.1% | 225 | 92.6% |
| Southern | 446 | 439 | 98.4% | 426 | 95.5% |
| Western | 312 | 297 | 95.2% | 294 | 94.1% |
| Urban | 1,347 | 1,333 | 99.0% | 1,222 | 90.7% |
| Rural | 2,789 | 2,711 | 97.2% | 2,518 | 90.3% |
| Lowest 40% | 1,785 | 1,724 | 96.6% | 1,585 | 88.8% |
| Highest 40% | 1,513 | 1,501 | 99.2% | 1,380 | 91.2% |
| National Average | 4,136 | 4,044 | 97.8% | 3,739 | 90.4% |
Figure 4. ANC Distribution of IFA Tablets: Number of Tablets Received and Taken According to Number of ANC Visits, Zambia, 2007

Figure 5. Relative Importance of Each Falter Point in Zambia: Why Women Who Were Pregnant in the Last Five Years Failed to Take the Ideal Minimum of 180 IFA Tablets
Footnotes
1 WHO categorizes the severity of anemia as a public health problem according to the condition’s prevalence: < 5 percent, no public health problem; 5–19.9 percent, mild; 20–39.9 percent, moderate; ≥ 40 percent, severe.
2 The ZDHS asked about IFA tablets or capsules; this brief refers to all forms as “tablets.”
3 The ZDHS provides a population-based, nationally representative sample of all women in Zambia.
References
Fleming, A. F. 1989. “The Aetiology of Severe Anaemia in Pregnancy in Ndola, Zambia.” Annals of Tropical Medicine and Parasitology 83(1): 37–49.
Central Statistical Office (CSO), Central Board of Health (CBH) [Zambia], and ORC Macro. 2003. Zambia Demographic and Health Survey 2001–2002. Calverton, MD: CSO, CBH, and ORC Macro.
Central Statistical Office (CSO), Ministry of Health (MOH) [Zambia], Tropical Diseases Research Centre (TDRC), University of Zambia, and Macro International. 2009. Zambia Demographic and Health Survey 2007. Calverton, MD: CSO and Macro International.
Horton, S., and J. Ross. 2003. “The Economics of Iron Deficiency.” Food Policy 28(1):51–75.
Luo, C., C. M. Mwela, and J. Campbell. 1999. National Baseline Survey on Prevalence and Aetiology of Anaemia in Zambia: A Random Cluster Community Survey Involving Children, Women and Men. Lusaka: National Food and Nutrition Commission.
Ministry of Health (MOH) [Zambia]. 2010. National Health and Strategic Plan 2011–2015. Lusaka: Government of Zambia.
Stoltzfus, R. J., and M. L. Dreyfuss. 1998. Guidelines for the Use of Iron Supplements to Prevent and Treat Iron Deficiency Anemia. Washington, DC: ILSI Press.
Stoltzfus, R. J., L. Mullany, and R. E. Black. 2004. “Iron Deficiency Anemia.” In Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors. M. Ezzati, A. D. Lopez, A. Rodgers, and C. J. L. Murray, eds. Geneva: World Health Organization.
United Nations Development Programme (UNDP). 2013. Millennium Development Goals Progress Report, Zambia, 2013. Lusaka: UNDP.
World Health Organization (WHO). 2012. “Guideline: Daily Iron and Folic Acid Supplementation in Pregnant Women.” Geneva: WHO.